

Trends in Early-Onset Colorectal Cancer in Singapore: Epidemiological Study of a Multiethnic Population
- PMID: 39725547
- PMCID: PMC11888020
- DOI: 10.2196/62835
Trends in Early-Onset Colorectal Cancer in Singapore: Epidemiological Study of a Multiethnic Population
Abstract
Background: Colorectal cancer (CRC) incidence and mortality in those aged 50 years and above have decreased over the past 2 decades. However, there is a rising incidence of CRC among individuals under 50 years of age, termed early-onset colorectal cancer (EOCRC). Patients with EOCRC are diagnosed at an advanced stage and may be in more psychosocial, emotional, and financial distress.
Objective: Our study examined the epidemiological shifts in CRC in Singapore, a multiethnic country.
Methods: CRCs diagnosed at age 20 years and above were identified from the Singapore Cancer Registry (SCR) from 1968 to 2019. Patient characteristics included gender, ethnicity, and age of CRC diagnosis. Population information was obtained from the Department of Statistics Singapore (SingStat). Age-specific incidence rates (ASRs) and age-standardized incidence rates (ASIRs) were calculated. The cohort was divided into 3 age groups: 20-49, 50-64, and ≥65 years. Temporal trends in incidence rates were modeled with joinpoint regression. Birth cohort models were fitted using the National Cancer Institute (NCI) age-period-cohort analysis tool. Cancer-specific survival analysis was performed with the Cox proportional hazards model.
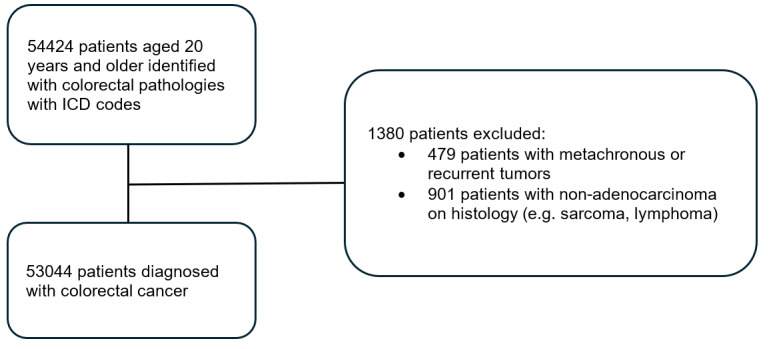
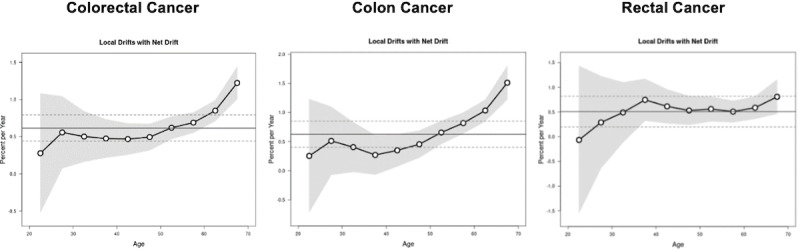
Results: In total, 53,044 CRCs were included, and 6183 (11.7%) adults aged 20-49 years were diagnosed with EOCRC. The ASR of EOCRC rose from 5 per 100,000 population in 1968 to 9 per 100,000 population in 1996 at 2.1% annually and rose to 10 per 100,000 population in 2019 at 0.64% annually. The ASR for CRC among adults aged 50-64 years rose at 3% annually from 1968 to 1987 and plateaued from 1987, while the ASR for adults aged 65 years and above rose at 4.1% annually from 1968 to 1989 and 1.3% annually from 1989 to 2003 but decreased from 2003 onwards at 1% annually. The ASR of early-onset rectal cancer increased significantly at 1.5% annually. There was a continued rise in the ASR of EOCRC among males (annual percentage change [APC] 1.5%) compared to females (APC 0.41%). Compared to the 1950-1954 reference birth cohort, the 1970-1984 birth cohort had a significantly higher incidence rate ratio (IRR) of 1.17-1.36 for rectal cancer, while there was no significant change for colon cancer in later cohorts. There were differences in CRC trends across the 3 ethnic groups: Malays had a rapid and persistent rise in the ASR of CRC across all age groups (APC 1.4%-3%), while among young Chinese, only the ASR of rectal cancer was increasing (APC 1.5%). Patients with EOCRC had better survival compared to patients diagnosed at 65 years and above (hazard ratio [HR] 0.73, 95% CI 0.67-0.79, P<.001) after adjusting for covariates.
Conclusions: The rise in the incidence of rectal cancer among young adults, especially among Chinese and Malays, in Singapore highlights the need for further research to diagnose CRC earlier and reduce cancer-related morbidity and mortality.
Keywords: Singapore; age-period-cohort; early-onset colorectal cancer; epidemiology; health disparity; joinpoint regression; public health.
©Hui Lionel Raphael Chen, Qingqing Dawn Chong, Brenda Tay, Siqin Zhou, Evelyn Yi Ting Wong, Isaac Seow-En, Ker Kan Tan, Yi Wang, Adeline Seow, Kwong-Wei Emile Tan, Bee Huat Iain Tan, Sze Huey Tan. Originally published in JMIR Public Health and Surveillance (https://publichealth.jmir.org), 14.02.2025.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures







References
-
- Xi Y, Xu P. Global colorectal cancer burden in 2020 and projections to 2040. Transl Oncol. 2021 Oct;14(10):101174. doi: 10.1016/j.tranon.2021.101174. https://linkinghub.elsevier.com/retrieve/pii/S1936-5233(21)00166-2 S1936-5233(21)00166-2 - DOI - PMC - PubMed
-
- Sung H, Siegel RL, Laversanne M, Jiang C, Morgan E, Zahwe M, Cao Y, Bray F, Jemal A. Colorectal cancer incidence trends in younger versus older adults: an analysis of population-based cancer registry data. Lancet Oncol. 2024 Dec 11;:S1470-2045. doi: 10.1016/S1470-2045(24)00600-4. https://linkinghub.elsevier.com/retrieve/pii/S1470-2045(24)00600-4 S1470-2045(24)00600-4 - DOI - PMC - PubMed
-
- Siegel RL, Wagle NS, Cercek A, Smith RA, Jemal A. Colorectal cancer statistics, 2023. CA Cancer J Clin. 2023;73(3):233–254. doi: 10.3322/caac.21772. https://onlinelibrary.wiley.com/doi/10.3322/caac.21772 - DOI - PubMed
-
- Feletto E, Yu XQ, Lew J, St John DJB, Jenkins MA, Macrae FA, Mahady SE, Canfell K. Trends in colon and rectal cancer incidence in Australia from 1982 to 2014: analysis of data on over 375,000 cases. Cancer Epidemiol Biomarkers Prev. 2019 Jan;28(1):83–90. doi: 10.1158/1055-9965.EPI-18-0523.1055-9965.EPI-18-0523 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
