

Effect of individualized versus conventional perioperative blood pressure management on postoperative major complications in high-risk patients undergoing noncardiac surgery: study protocol for the SPROUT-4 multicenter randomized controlled trial
- PMID: 39725988
- PMCID: PMC11673592
- DOI: 10.1186/s13063-024-08707-4
Effect of individualized versus conventional perioperative blood pressure management on postoperative major complications in high-risk patients undergoing noncardiac surgery: study protocol for the SPROUT-4 multicenter randomized controlled trial
Abstract
Background: Intraoperative hypotension is very common during surgery and is linked to major organ dysfunction and mortality. Current perioperative blood pressure management is largely based on universal blood pressure thresholds ranging from a mean arterial pressure of 60-70 mmHg. However, the effectiveness of this conventional management remains unproven in prospective randomized trials. Therefore, we will conduct this study to test if individualized perioperative blood pressure management decreases the incidence of postoperative major adverse outcomes.
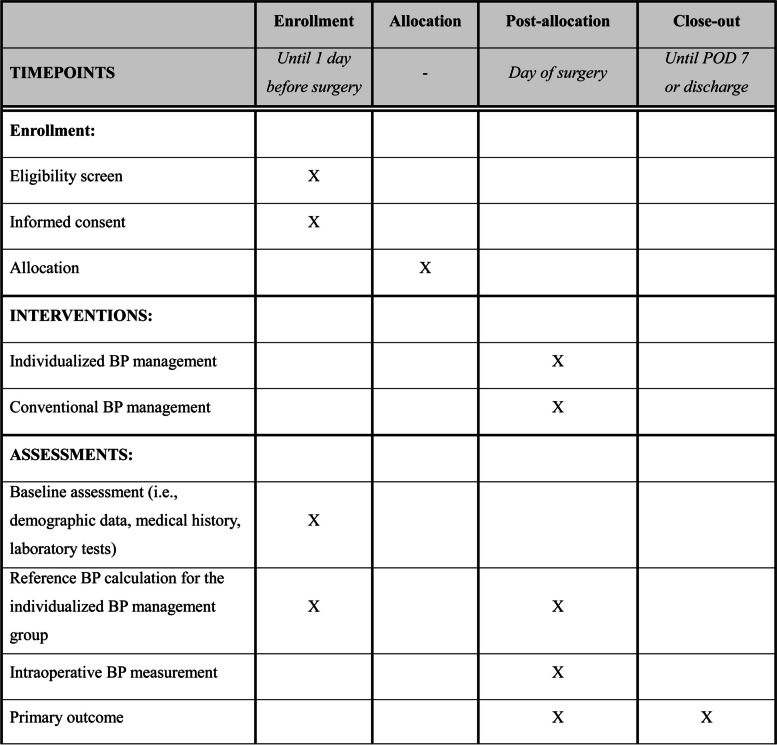
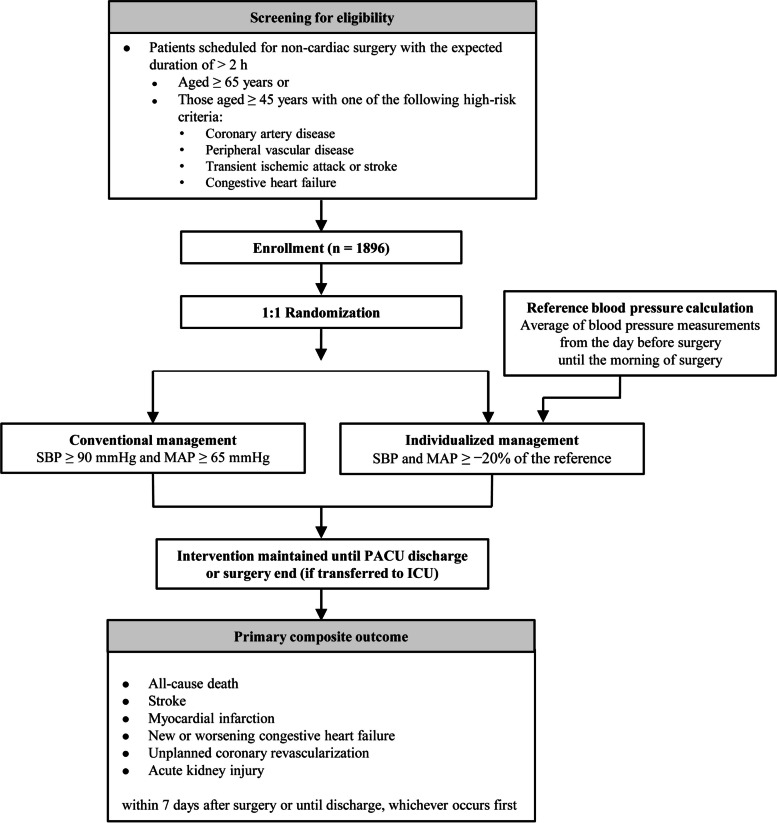
Methods: This multicenter, randomized controlled superiority trial will enroll 1896 high-risk patients undergoing major noncardiac surgery from five tertiary university hospitals in South Korea. In the control group, mean arterial pressure will be maintained at ≥ 65 mmHg and systolic blood pressure ≥ 90 mmHg during surgery. In the intervention group, mean arterial pressure and systolic blood pressure will be maintained at no less than 20% of their baseline values. The baseline values are calculated as the average of all values measured from the day before surgery until the morning of surgery. These targets will be maintained until the patient is discharged from the post-anesthesia care unit or, for those who are transferred to the intensive care unit after surgery, until the end of the surgery. No specific restrictions, except for these blood pressure targets, will be applied to perioperative management. The primary composite outcome consists of all-cause death, stroke, myocardial infarction, new or worsening congestive heart failure, unplanned coronary revascularization, and acute kidney injury within 7 days after noncardiac surgery or until hospital discharge, whichever occurs first.
Discussion: This study will reveal if individualized perioperative blood pressure management decreases the risk of major adverse outcomes in patients at high-risk undergoing noncardiac surgery.
Trial registration: ClinicalTrials.gov NCT06225453. Registered on January 26, 2024.
Keywords: Anesthesia; Blood pressure; Hypotension; Postoperative complications; Randomized controlled trial.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol was reviewed and approved by the Institutional Review Boards of the five participating hospitals (Ajou University Medical Center, No. AJOUIRB-IV-2024–042 on January 22, 2024; Korea University Guro Hospital, No. 2024GR0016 on January 4, 2024; Samsung Medical Center, No. 2023–12-098–001 on February 15, 2024; Seoul National University Bundang Hospital, No. B-2402–883-402 on February 2, 2024; Seoul National University Hospital, No. 2312–127-1496 on January 10, 2024). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Salmasi V, Maheshwari K, Yang D, Mascha EJ, Singh A, Sessler DI, et al. Relationship between intraoperative hypotension, defined by either reduction from baseline or absolute thresholds, and acute kidney and myocardial injury after noncardiac surgery: a retrospective cohort analysis. Anesthesiology. 2017;126:47–65. 10.1097/ALN.0000000000001432. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
