

Diagnosis and treatment experience of cecal diverticulitis in six pediatric patients
- PMID: 39726533
- PMCID: PMC11669651
- DOI: 10.3389/fped.2024.1478296
Diagnosis and treatment experience of cecal diverticulitis in six pediatric patients
Abstract
Objective: This study aims to summarize the clinical characteristics, diagnostic methods, and treatment experience of cecal diverticulitis in children.
Method: The clinical data of six pediatric patients with cecal diverticulitis, treated at Children's Hospital Affiliated to Shandong University from November 2021 to May 2023, were retrospectively analyzed.
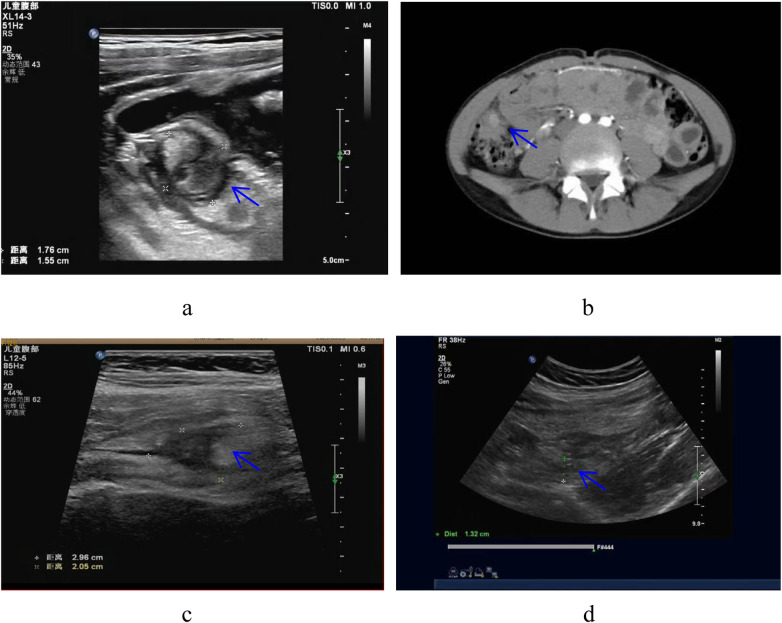
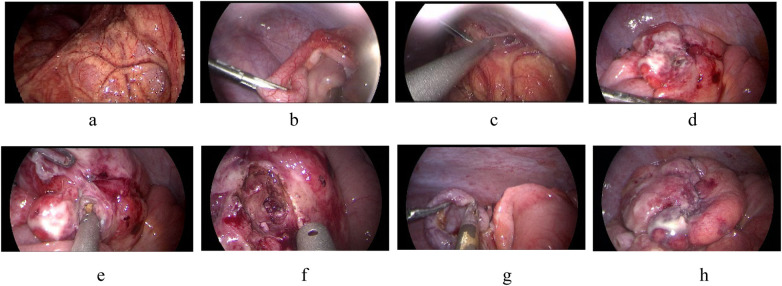
Result: All patients presented with abdominal pain primarily in the lower right abdomen. Two cases had fever with a maximum body temperature not exceeding 38.0°C. Three cases exhibited elevated inflammatory markers such as white blood cell count and C-reactive protein (CRP) upon admission. Three children were misdiagnosed with acute appendicitis based on preoperative color Doppler ultrasound. Two children were treated with third-generation cephalosporins and ornidazole for anti-inflammatory therapy and were cured after 6 and 9 days of hospitalization, respectively. Four children underwent laparoscopic surgery with excision of the cecal diverticulum and cecal repair, all of whom recovered well without postoperative complications. The operation duration ranged from 100 to 170 min, with an average of 140 min. Intraoperative blood loss ranged from 5 to 10 ml, averaging 6.75 ml. The overall length of hospital stay was 8-12 days, with an average stay of 9.5 days. All patients were followed up until December 2023, with no recurrences observed.
Conclusion: Children with cecal diverticulitis, especially complex cecal diverticulitis, are easily misdiagnosed as acute appendicitis. Acute simple cecal diverticulitis can be treated with anti-inflammatory therapy. Laparoscopic cecal diverticulectomy combined with cecal repair is a feasible and effective method for treating acute complex cecal diverticulitis.
Keywords: cecal diverticulitis; children; clinical characteristics; diagnosis; treatment.
© 2024 Li, Liu, Zhang and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous