

Quality of pediatric trauma care: development of an age-adjusted TRISS model and survival benchmarking in a major trauma center
- PMID: 39726535
- PMCID: PMC11669499
- DOI: 10.3389/fped.2024.1481467
Quality of pediatric trauma care: development of an age-adjusted TRISS model and survival benchmarking in a major trauma center
Abstract
Background: Pediatric trauma is a major global health concern, accounting for a substantial proportion of deaths and disease burden from age 5 onwards. Effective triage and management are essential in pediatric trauma care, and prediction models such as the Trauma Injury Severity Score (TRISS) play a crucial role in estimating survival probability and guiding quality improvement. However, TRISS does not account for age-specific factors in pediatric populations, limiting its applicability to younger patients. This study aimed to modify TRISS to account for age for children (Peds-TRISS) and to evaluate its performance relative to the original TRISS. We also assessed survival outcomes to explore the model's potential utility across various clinical settings. These efforts align with quality improvement initiatives to reduce preventable mortality and supporting sustainable development goals.
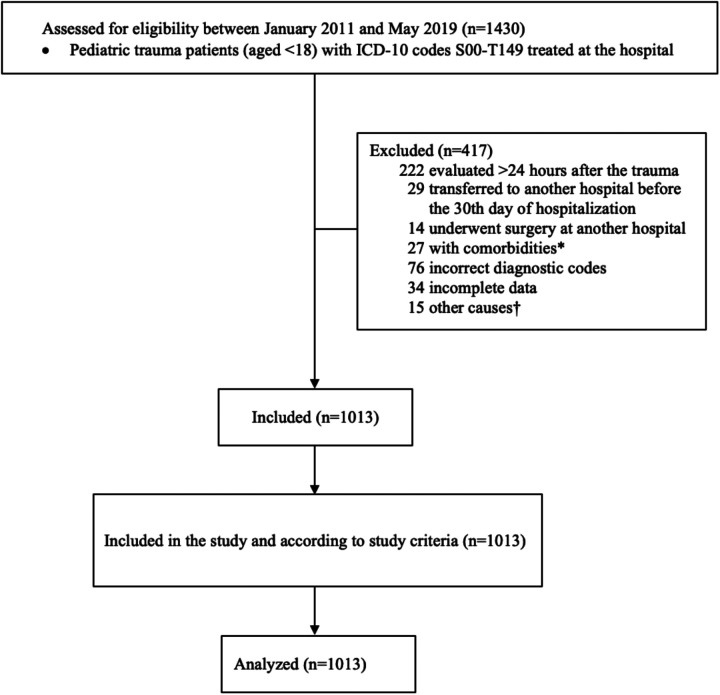
Methods: This retrospective cohort study included patients under 18 years of age who were treated at a hospital in Colombia between 2011 and 2019. New coefficients for TRISS covariates were calculated using logistic regression, with age treated as a continuous variable. Model performance was evaluated based on discrimination (C statistic) and calibration, comparing Peds-TRISS with the original TRISS. Internal validation was conducted using bootstrap resampling. Survival outcomes were assessed using the M and Z statistics, which are commonly used for international trauma outcome comparisons.
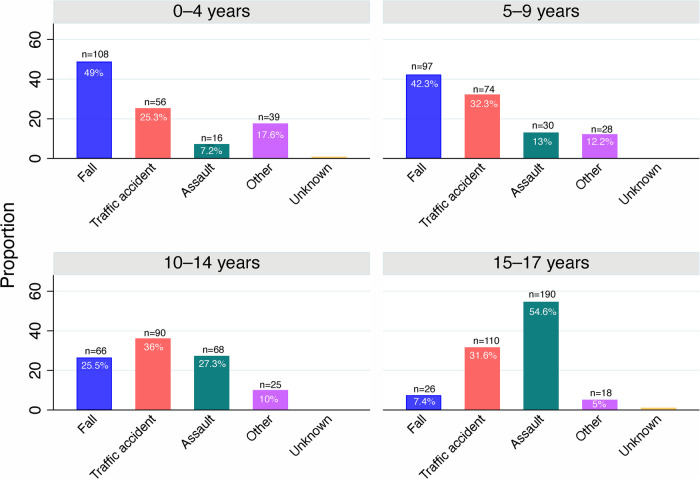
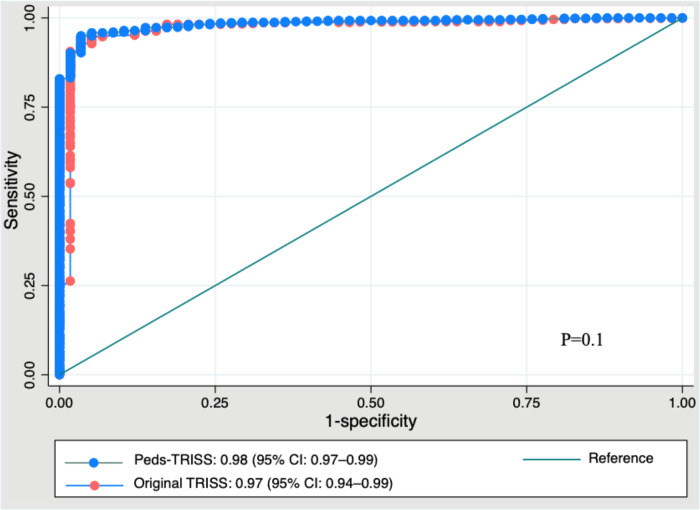
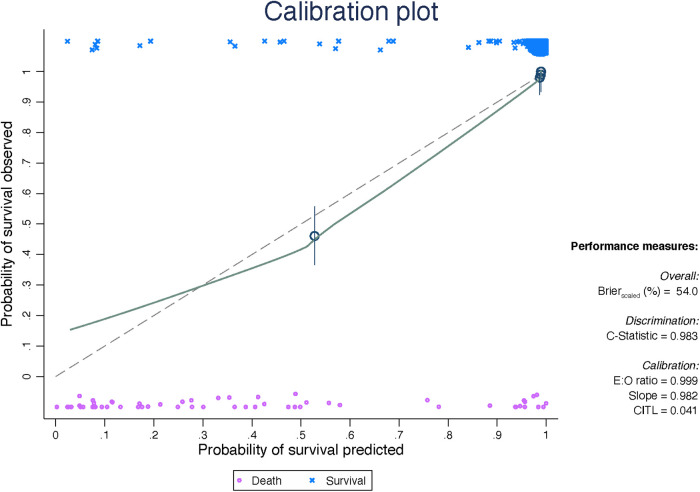
Results: The study included 1,013 pediatric patients with a median age of 12 years (IQR 5-15), of whom 73% were male. The leading causes of injury were traffic accidents (31.1%), falls (28.8%), and assaults (28.7%). The overall mortality rate was 5.7%. The Peds-TRISS model demonstrated good calibration (HL = 9.7, p = 0.3) and discrimination (C statistic = 0.98, 95% CI 0.97-0.99), with no statistically significant difference in the ROC curve comparison with the original TRISS. Internal validation demonstrated strong performance of Peds-TRISS. The M and Z statistics were 0.93 and 0, respectively, indicating no significant differences between expected and observed survival rates.
Conclusions: Most fatalities occurred among adolescents and were due to intentional injuries. The Peds-TRISS model showed a partial improvement in performance compared to the original TRISS, with superior results in terms of calibration, although not in discrimination. These findings highlight the potential of model customization for specific populations. Prospective, multicenter studies are recommended to further validate the model's utility across diverse settings.
Keywords: TRISS; injuries; pediatric trauma; quality of care; survival prediction; trauma injury severity score; trauma score; trauma severity indices.
© 2024 De los Ríos-Pérez, García, Gomez, Arias and Fandiño-Losada.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- UNICEF. For Every Child. Child and Adolescent Injuries. New York, NY: UNICEF; (2020). Available online at: https://www.unicef.org/health/injuries#:∼:text=Globally%2C%20more%20than... (accessed October 31, 2024).
-
- World Health Organization. Urges More Effective Prevention of Injuries and Violence Causing 1 in 12 Deaths Worldwide. Geneva: The World Health Organization (WHO) (2022). Available online at: https://www.who.int/news/item/29-11-2022-who-urges-more-effective-preven... (accessed April 13, 2024).
-
- Institute for Health Metrics and Evaluation (IHME). GBD Compare Data Visualization. Seattle, WA: IHME, University of Washington; (2024). Available online at: http://vizhub.healthdata.org/gbd-compare (accessed June 13, 2024).
-
- Global Health Estimates 2021. Deaths by Cause, Age, Sex, by Country and by Region, 2000–2021. Geneva, World Health Organization; (2024). Available online at: https://www.who.int/data/gho/data/themes/mortality-and-global-health-est... (accessed July 1, 2024).
LinkOut - more resources
Full Text Sources