

Haemodynamic and hyperaemic effects of adenosine in patients with atrial fibrillation undergoing quantitative myocardial perfusion cardiovascular magnetic resonance
- PMID: 39726566
- PMCID: PMC11670251
- DOI: 10.1093/ehjimp/qyae127
Haemodynamic and hyperaemic effects of adenosine in patients with atrial fibrillation undergoing quantitative myocardial perfusion cardiovascular magnetic resonance
Abstract
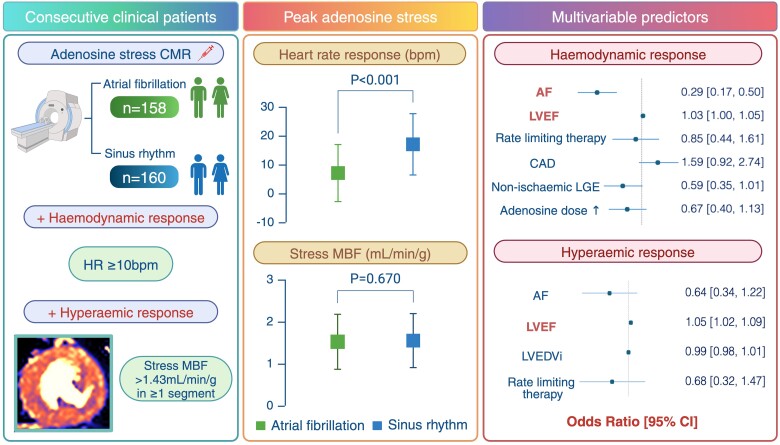
Aims: Patients with atrial fibrillation (AF) are thought to have an attenuated response to adenosine during vasodilator stress testing. We sought to investigate the haemodynamic and hyperaemic effects of adenosine in patients with AF undergoing adenosine-stress cardiovascular magnetic resonance (CMR) assessment.
Methods and results: We retrospectively examined 318 patients referred for clinical adenosine-stress CMR (AF n = 158, sinus rhythm [SR] n = 160). Baseline and peak heart rate (HR) and quantitative myocardial perfusion were compared between groups. At peak stress, the haemodynamic response was blunted in patients with AF (HR increase 7 ± 10bpm vs. 17 ± 11bpm in SR, P < 0.001). Fewer patients in AF met the threshold for a satisfactory HR response ≥10bpm (40% in AF vs. 76% in SR, P < 0.001). There were no intergroup differences in hyperaemic myocardial blood flow (1.52 ± 0.65 mL/min/g in AF vs. 1.55 ± 0.65 mL/min/g in SR, P = 0.670) or myocardial perfusion reserve (2.66 ± 1.11 in AF vs. 2.66 ± 1.08 in SR, P = 0.981). AF (odds ratio [OR], 0.29 [0.17-0.50], P < 0.001) and left ventricular ejection fraction (OR 1.03 [1.00-1.05], P = 0.023) were independently associated with achieving a satisfactory HR response on multivariable analysis, but only ejection fraction (OR 1.05 [1.02-1.09], P = 0.003) predicted a satisfactory hyperaemic response.
Conclusion: The heart rate response during adenosine-stress CMR is blunted in AF patients. Despite this, the majority of patients with AF generate a sufficient hyperaemic response with a standard adenosine-stress protocol. Further work is needed to determine the diagnostic accuracy of adenosine-stress CMR in patients with AF.
Keywords: adenosine; atrial fibrillation; cardiovascular magnetic resonance; hyperaemic myocardial blood flow; left ventricular systolic dysfunction; stress perfusion.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: The authors declare that they have no competing interests.
Figures
 A 77-year-old male with persistent atrial fibrillation and recurrent chest pain with absent haemodynamic response to 170µg/kg/min of adenosine (baseline; heart rate, 94bpm, blood pressure, 127/85mmHg; and peak stress, 91bpm, 123/80mmHg). No perfusion defects are appreciated on qualitative assessment of raw stress perfusion images (Panel B), but pixel-wise myocardial blood flow perfusion maps (Panel A) and polar plot (Panel C) confirm adequate hyperaemia at all three left ventricular levels. Case 2
A 77-year-old male with persistent atrial fibrillation and recurrent chest pain with absent haemodynamic response to 170µg/kg/min of adenosine (baseline; heart rate, 94bpm, blood pressure, 127/85mmHg; and peak stress, 91bpm, 123/80mmHg). No perfusion defects are appreciated on qualitative assessment of raw stress perfusion images (Panel B), but pixel-wise myocardial blood flow perfusion maps (Panel A) and polar plot (Panel C) confirm adequate hyperaemia at all three left ventricular levels. Case 2  A 67-year-old male with persistent atrial fibrillation and severe left ventricular systolic dysfunction referred for investigation of recurrent angina: absent haemodynamic response to high-dose (210µg/kg/min) adenosine (baseline; heart rate, 85bpm; blood pressure, 129/78mmHg; peak stress, 85bpm, 124/63mmHg). Pixel-wise hyperaemic maps (Panel A) and raw perfusion sequences (Panel C) show a perfusion defect in the right coronary artery territory with a corresponding regional reduction in hyperaemic myocardial blood flow (Panel B) with evidence of adequate hyperaemia in the unaffected myocardial segments. The perfusion defect significantly exceeded the areas of infarction detected on phase-sensitive inversion recovery late gadolinium enhancement images (Panel D). Invasive coronary angiography demonstrating an occluded mid-right coronary artery with collateralisation from the left coronary system (Panel E).
A 67-year-old male with persistent atrial fibrillation and severe left ventricular systolic dysfunction referred for investigation of recurrent angina: absent haemodynamic response to high-dose (210µg/kg/min) adenosine (baseline; heart rate, 85bpm; blood pressure, 129/78mmHg; peak stress, 85bpm, 124/63mmHg). Pixel-wise hyperaemic maps (Panel A) and raw perfusion sequences (Panel C) show a perfusion defect in the right coronary artery territory with a corresponding regional reduction in hyperaemic myocardial blood flow (Panel B) with evidence of adequate hyperaemia in the unaffected myocardial segments. The perfusion defect significantly exceeded the areas of infarction detected on phase-sensitive inversion recovery late gadolinium enhancement images (Panel D). Invasive coronary angiography demonstrating an occluded mid-right coronary artery with collateralisation from the left coronary system (Panel E).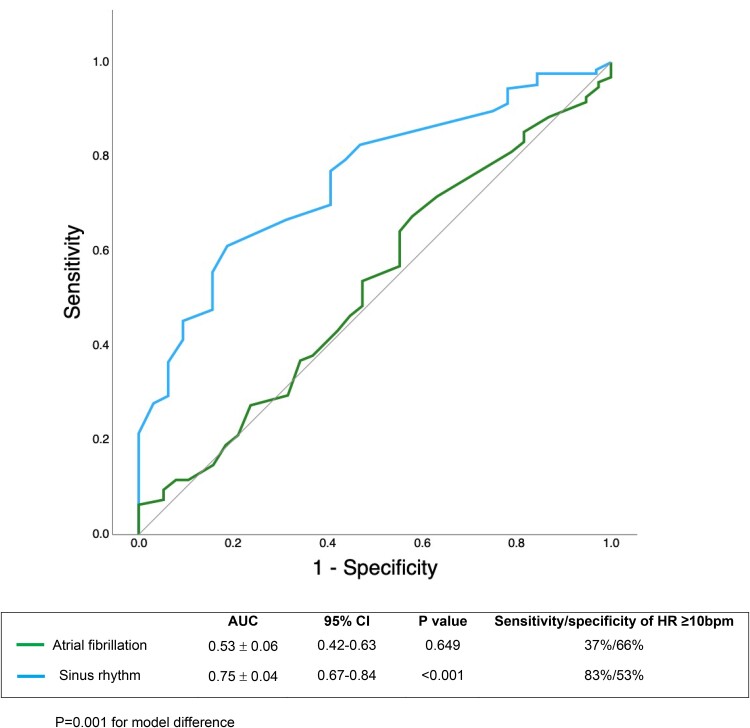
Similar articles
-
Assessing splenic switch-off in Adenosine stress CMR for patients with atrial fibrillation: a propensity-matched study.Br J Radiol. 2022 Oct 1;95(1139):20220422. doi: 10.1259/bjr.20220422. Epub 2022 Sep 26. Br J Radiol. 2022. PMID: 36000672 Free PMC article.
-
Guiding early revascularization using [15O]H2O positron emission tomography myocardial perfusion imaging: impact of atrial fibrillation.Eur Heart J Cardiovasc Imaging. 2024 Jun 28;25(7):958-967. doi: 10.1093/ehjci/jeae043. Eur Heart J Cardiovasc Imaging. 2024. PMID: 38376457
-
Quantitative cardiovascular magnetic resonance myocardial perfusion mapping to assess hyperaemic response to adenosine stress.Eur Heart J Cardiovasc Imaging. 2021 Feb 22;22(3):273-281. doi: 10.1093/ehjci/jeaa252. Eur Heart J Cardiovasc Imaging. 2021. PMID: 33188683 Free PMC article.
-
An acute increase in Left Atrial volume and left ventricular filling pressure during Adenosine administered myocardial hyperaemia: CMR First-Pass Perfusion Study.BMC Cardiovasc Disord. 2023 May 11;23(1):246. doi: 10.1186/s12872-023-03230-x. BMC Cardiovasc Disord. 2023. PMID: 37170253 Free PMC article.
-
Feasibility and safety of high-dose adenosine perfusion cardiovascular magnetic resonance.J Cardiovasc Magn Reson. 2010 Nov 16;12(1):66. doi: 10.1186/1532-429X-12-66. J Cardiovasc Magn Reson. 2010. PMID: 21080924 Free PMC article.
References
-
- Schwitter J, Wacker CM, van Rossum AC, Lombardi M, Al-Saadi N, Ahlstrom H et al. MR-IMPACT: comparison of perfusion-cardiac magnetic resonance with single-photon emission computed tomography for the detection of coronary artery disease in a multicentre, multivendor, randomized trial. Eur Heart J 2008;29:480–9. - PubMed
-
- Watkins S, McGeoch R, Lyne J, Steedman T, Good R, McLaughlin MJ et al. Validation of magnetic resonance myocardial perfusion imaging with fractional flow reserve for the detection of significant coronary heart disease. Circulation 2009;120:2207–13. - PubMed
-
- Schwitter J, Wacker CM, Wilke N, Al-Saadi N, Sauer E, Huettle K et al. MR-IMPACT II: magnetic resonance imaging for myocardial perfusion assessment in coronary artery disease trial: perfusion-cardiac magnetic resonance vs. single-photon emission computed tomography for the detection of coronary artery disease: a comparative multicentre, multivendor trial. Eur Heart J 2013;34:775–81. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous