

Maternal and pregnancy factors contributing to the association between area deprivation and infant mortality in England: a retrospective cohort study
- PMID: 39726725
- PMCID: PMC11670682
- DOI: 10.1016/j.lanepe.2024.101075
Maternal and pregnancy factors contributing to the association between area deprivation and infant mortality in England: a retrospective cohort study
Abstract
Background: Socioeconomic inequality in infant mortality in the UK is rising. This study aims to identify contributory maternal and pregnancy factors that can explain the known association between area deprivation and infant mortality.
Methods: A cohort study was conducted using Clinical Practice Research Datalink (CPRD) primary care data between 2004 and 2019 linked to the Index of Multiple Deprivation (IMD), and infant mortality from the Office for National Statistics death data. Potential maternal and pregnancy contributory factors included: maternal age, prior maternal health conditions, pregnancy lifestyle factors and complications, use of medications during pregnancy, and characteristics of birth. Counterfactual-based decomposition analysis was used to quantify the relative importance of equalising these factors to reduce inequalities in infant mortality.
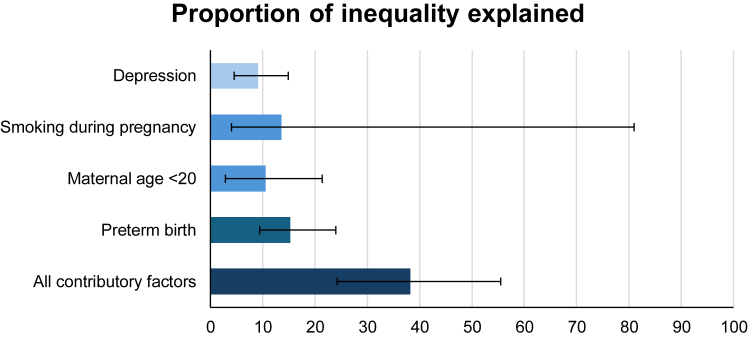
Findings: A total of 392,606 mother-child dyads were included in this study. The overall risk of infant mortality was greatest for individuals in the most deprived quintile (risk ratio 2.13 [95% CI 1.58-2.90]; risk difference 6.6 [3.8-8.8] per 10,000 live births) compared with the least deprived. Four contributory factors were identified as potentially important: preterm birth (Proportion eliminated [PE] 15.25% [95% CI 9.44-24.12%]), smoking during pregnancy (PE 13.61% [95% CI 3.96-80.97%]), maternal age <20 years at childbirth (PE 10.52% [95% CI 2.93-21.35%]) and maternal depression (PE 9.13% [95% CI 4.47-14.93%]). These collectively accounted for more than one-third of the socioeconomic inequality in mortality.
Interpretation: Multifactorial interventions targeting maternal mental health, smoking, teenage pregnancy and preterm birth may mitigate a proportion of the effects of socioeconomic inequality but targeting these, alone, will not stem the rise in infant mortality. Structural efforts to reduce socioeconomic inequalities will also be required to prevent these excess infant deaths.
Funding: UK Medical Research Council, Scottish Chief Scientist Office, Wellcome Trust.
Keywords: Cohort study; Health inequality; Infant mortality; Socioeconomic deprivation.
© 2024 The Author(s).
Conflict of interest statement
FH received research funding from Glasgow Children Hospital Charity, Biotechnology and Biological Sciences Research Council, Understanding Children's Trust, and The Swedish Child Neuropsychiatry Science Foundation, consulting fee from the Chinese University of Hong Kong, and personal honorarium from Sage Publications. KM received research funding from CW Maplethorpe Fellowship, European Commission Horizon 2020, National Institute for Health and Care Research UK, Hong Kong Research Grant Council. JC received research funding from Bristol Myers Squibb, CSL-Vifor, British Heart Foundation, and Pharmacosmos, consulting fee from Pharmacosmos, CSL-Vifor, and Biopeutics, personal honorarium from Pharmacosmos and ABBOTT, travel support from Pharmacosmos, participated on advisory boards of Medtronic, ADAPT-CRT, CMR-Guide, PROTECT-HF, and have stocks or stock options in HeartFelt (non-invasive monitoring), Viscardia (synchronous diaphragmatic pacing). CD received research funding from Wellcome Trust. PI received research funding from Hong Kong Health and Medical Research Fund and Hong Kong General Research Fund. ICKW received research grants from Amgen, Janssen, GSK, Novartis, Pfizer, Bayer and Bristol-Myers Squibb and Takeda, Institute for Health Research in England, European Commission, National Health and Medical Research Council in Australia, The European Union's Seventh Framework Programme for research, technological development, Research Grants Council Hong Kong and Health and Medical Research Fund Hong Kong; consulting fees from IQVIA and World Health Organization; payment for expert testimony for Appeal Court in Hong Kong; serves on advisory committees for Member of Pharmacy and Poisons Board; is a member of the Expert Committee on Clinical Events Assessment Following COVID-19 Immunization; is a member of the Advisory Panel on COVID-19 Vaccines of the Hong Kong Government; is the non-executive director of Jacobson Medical in Hong Kong; and is the founder and director of Therakind Limited (UK), Advance Data Analytics for Medical Science (ADAMS) Limited (HK), Asia Medicine Regulatory Affairs (AMERA) Services Limited and OCUS Innovation Limited (HK, Ireland and UK). PW received research funding from Boehringer Ingelheim, Astrazeneca, Roche diagnostics, Novartis, personal honorarium from Novo Nordisk and Raisio. AP received research funding from Wellcome Trust, MRC, CSO, NIHR, Obesity Action Scotland, Health Foundation, and UKPRP.
Figures

Similar articles
-
Adverse pregnancy outcomes attributable to socioeconomic and ethnic inequalities in England: a national cohort study.Lancet. 2021 Nov 20;398(10314):1905-1912. doi: 10.1016/S0140-6736(21)01595-6. Epub 2021 Nov 1. Lancet. 2021. PMID: 34735797
-
Mediation of socioeconomic inequalities in preterm birth. A cohort analysis of Welsh linked data.Acta Obstet Gynecol Scand. 2025 Jun;104(6):1081-1091. doi: 10.1111/aogs.15101. Epub 2025 Apr 16. Acta Obstet Gynecol Scand. 2025. PMID: 40241312 Free PMC article.
-
Child mortality in England compared with Sweden: a birth cohort study.Lancet. 2018 May 19;391(10134):2008-2018. doi: 10.1016/S0140-6736(18)30670-6. Epub 2018 May 3. Lancet. 2018. PMID: 29731173 Free PMC article.
-
[SENTIERI - Epidemiological Study of Residents in National Priority Contaminated Sites. Sixth Report].Epidemiol Prev. 2023 Jan-Apr;47(1-2 Suppl 1):1-286. doi: 10.19191/EP23.1-2-S1.003. Epidemiol Prev. 2023. PMID: 36825373 Italian.
-
Multiple-micronutrient supplementation for women during pregnancy.Cochrane Database Syst Rev. 2019 Mar 14;3(3):CD004905. doi: 10.1002/14651858.CD004905.pub6. Cochrane Database Syst Rev. 2019. PMID: 30873598 Free PMC article.
Cited by
-
Global Trends in Analgesic Opioid Use in Pregnancy: A Retrospective Cohort Study.Anesthesiology. 2025 Jun 1;142(6):1100-1113. doi: 10.1097/ALN.0000000000005418. Epub 2025 Feb 13. Anesthesiology. 2025. PMID: 39946665 Free PMC article.
-
Monitoring Perinatal Health in Europe: Strengths and Challenges of the Euro-Peristat Project.Paediatr Perinat Epidemiol. 2025 Jul;39(5):417-419. doi: 10.1111/ppe.70024. Epub 2025 Apr 20. Paediatr Perinat Epidemiol. 2025. PMID: 40254782 Free PMC article. No abstract available.
References
-
- House of Commons Library . 2023. Infant mortality and health inequalities.https://researchbriefings.files.parliament.uk/documents/CBP-9904/CBP-990...
-
- Office for National Statistics . Office for National Statistics; London: 2023. Child and infant mortality in England and Wales: 2021.
-
- Minnis H., Pollard A.P., Boyd K., et al. Academy of Medical Sciences; London: 2024. Prioritising early childhood to promote the nation's health, wellbeing and prosperity.
Grants and funding
LinkOut - more resources
Full Text Sources
