

Comparative Analysis of qSOFA, PRIEST, PAINT, and ISARIC4C Scores in Predicting Severe COVID-19 Outcomes Among Patients Aged over 75 Years
- PMID: 39727634
- PMCID: PMC11727413
- DOI: 10.3390/diseases12120304
Comparative Analysis of qSOFA, PRIEST, PAINT, and ISARIC4C Scores in Predicting Severe COVID-19 Outcomes Among Patients Aged over 75 Years
Abstract
Background: Elderly patients, particularly those over 75 years old, have been disproportionately affected by COVID-19, exhibiting higher rates of severe outcomes, such as ICU admissions and mortality. This study aimed to evaluate and compare the effectiveness of various clinical scoring systems-qSOFA, PRIEST, PAINT, and ISARIC4C-in predicting ICU admission, the need for mechanical ventilation, and mortality among elderly COVID-19 patients.
Methods: In this retrospective cohort study conducted at two tertiary care hospitals, 131 elderly patients (aged ≥ 75) and 226 younger controls (aged < 65) with confirmed COVID-19 were included. Clinical scores were computed at admission and five days after symptom onset. Kaplan-Meier survival analysis and Receiver Operating Characteristic (ROC) curve analysis were performed to assess the predictive performance of the scores regarding severe outcomes.
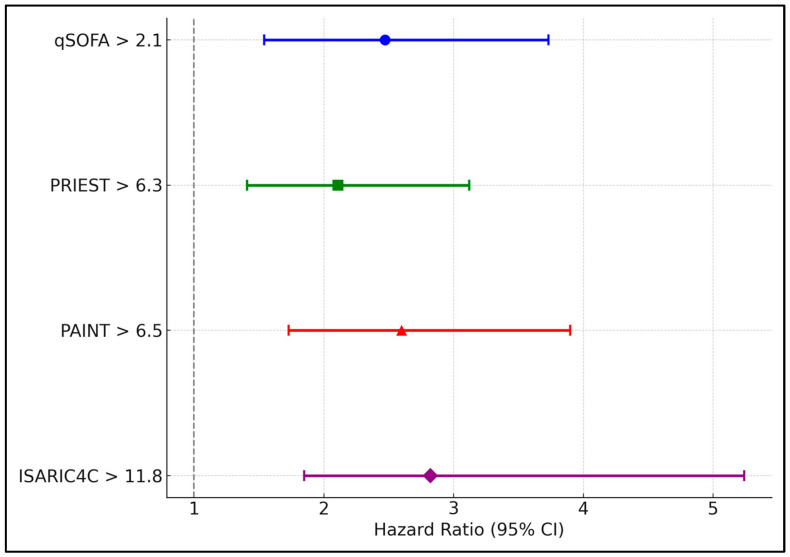
Results: Kaplan-Meier analysis indicated significantly lower survival probabilities for elderly patients with high scores at admission. Those with an ISARIC4C score above 11.8 had a survival probability of 25% compared to 74% for those below this threshold (p < 0.001). Similarly, elderly patients with a qSOFA score above 2.1 had a survival probability of 36% compared to 72% for those with lower scores (p < 0.001). The PRIEST and PAINT scores also demonstrated predictive validity; patients with a PRIEST score above 6.3 and a PAINT score above 6.5 at admission showed comparable decreases in survival probabilities. ROC analysis at five days post-symptom onset revealed that the ISARIC4C score had the highest area under the curve (AUC) of 0.772, suggesting excellent predictive validity for severe outcomes, including mortality. The optimal cutoffs identified were 11.2 for ISARIC4C, 6.3 for PRIEST, and 6.5 for PAINT, each displaying high sensitivity and specificity.
Conclusions: The ISARIC4C, qSOFA, PRIEST, and PAINT scores are robust predictors of severe outcomes in elderly COVID-19 patients over 75 years old, as confirmed by Kaplan-Meier and ROC analyses. These tools can be crucial for early identification of patients at high risk of adverse outcomes, guiding clinical decision making, and optimizing resource allocation. The use of these scoring systems should be encouraged in clinical settings to enhance the management of elderly COVID-19 patients. Further research is necessary to validate these findings across different populations and settings.
Keywords: COVID-19; ISARIC4C score; PAINT score; PRIEST score; elderly patients; mortality predictors; qSOFA.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
LinkOut - more resources
Full Text Sources
