

Management of Graves' upper eyelid retraction (GUER): A review
- PMID: 39728613
- PMCID: PMC11991553
- DOI: 10.4103/IJO.IJO_748_24
Management of Graves' upper eyelid retraction (GUER): A review
Abstract
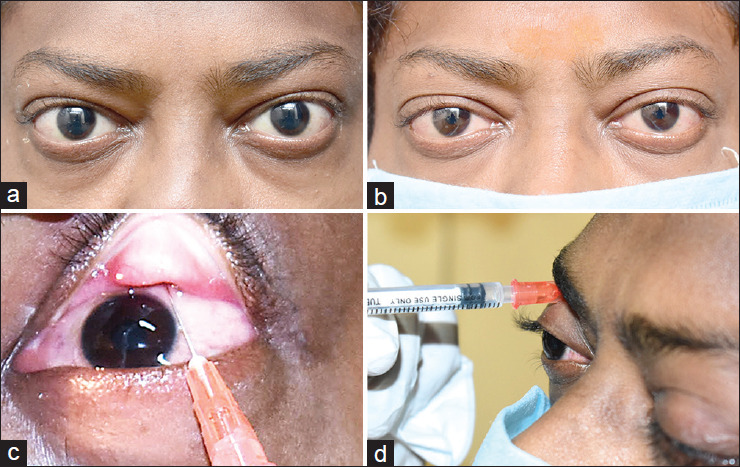
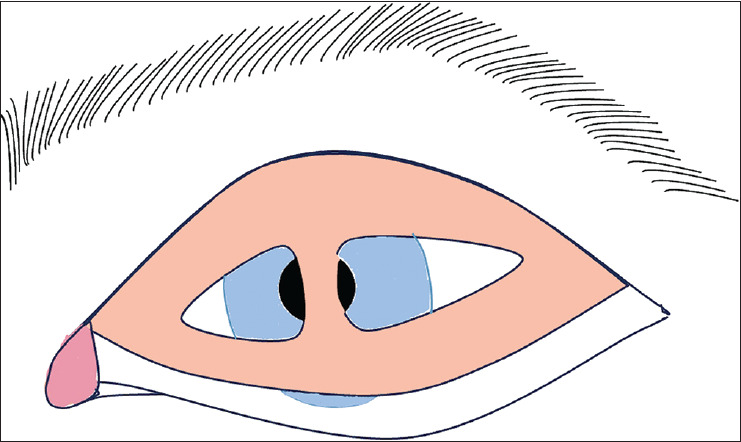
Graves' disease, a common autoimmune disorder, characteristically presents with upper eyelid retraction, causing significant functional and cosmetic concerns for affected individuals. The management of Graves' upper eyelid retraction has evolved significantly over recent years, with various surgical and non-surgical interventions. An ideal procedure is predictable and easily repeatable. This review provides a comprehensive overview of the contemporary approaches to managing Graves' upper eyelid retraction, encompassing both traditional and emerging techniques. It critically evaluates the surgical options for correcting Graves' upper eyelid retraction to achieve the desired eyelid contour, eyelid crease, tarsal platform show, and brow fat span. Their comparative effectiveness is meticulously explored, offering clinicians valuable insights into treatment selection. Moreover, this review also underscores combined orbital decompression with levator recession. Additionally, advancements in non-invasive modalities, including botulinum toxin, triamcinolone acetate injections, and hyaluronic acid fillers are discussed in detail. This review aims to facilitate informed decision-making and improve the overall outcomes for individuals affected by Graves' disease-associated upper eyelid retraction.
Copyright © 2024 Indian Journal of Ophthalmology.
Conflict of interest statement
There are no conflicts of interest.
Figures







References
-
- Goldstein I. Recession of the levator muscle for lagophthalmos in exophthalmic goiter. Arch Ophthalmol. 1934;11:389–93.
-
- Moran RE. The correction of exophthalmos and levator spasm. Plast Reconstr Surg. 1956;18:411–26. - PubMed
-
- Henderson JW. Relief of eyelid retraction: A surgical procedure. Arch Ophthalmol. 1965;74:205–16. - PubMed
-
- Putterman AM, Urist M. Surgical treatment of upper eyelid retraction. Arch Ophthalmol. 1972;87:401–5. - PubMed
-
- Putterman AM, Fett DR. Mueller’s muscle in the treatment of upper eyelid retraction: A 12-year study. Ophthalmic Surg. 1986;17:361–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
