

Effects of vaginal estrogen on serum estradiol during aromatase inhibitor therapy in breast cancer patients with vulvovaginal atrophy: a prospective trial
- PMID: 39729211
- PMCID: PMC11930867
- DOI: 10.1007/s10549-024-07564-8
Effects of vaginal estrogen on serum estradiol during aromatase inhibitor therapy in breast cancer patients with vulvovaginal atrophy: a prospective trial
Abstract
Purpose: This study aimed to analyze changes in serum estradiol (E2) levels during concurrent vaginal estradiol therapy and adjuvant letrozole in postmenopausal breast cancer (BC) patients with vulvovaginal atrophy (VVA). Secondary objectives included assessing the effects of therapy on vaginal atrophy, quality of life (QoL) and menopause-related symptoms.
Methods: 20 postmenopausal patients undergoing adjuvant letrozole therapy and experiencing VVA symptoms were treated with vaginal estradiol for 12 weeks. Gynecologic examination and symptom screening were conducted at baseline and after 12 weeks. Serum E2 levels were analyzed at baseline, and at two, four, eight, and 12 weeks. E2 levels were measured using both a routine liquid chromatography-tandem mass spectrometry (LC-MS/MS) method and a highly sensitive (hsE2-MS) LC-MS/MS method.
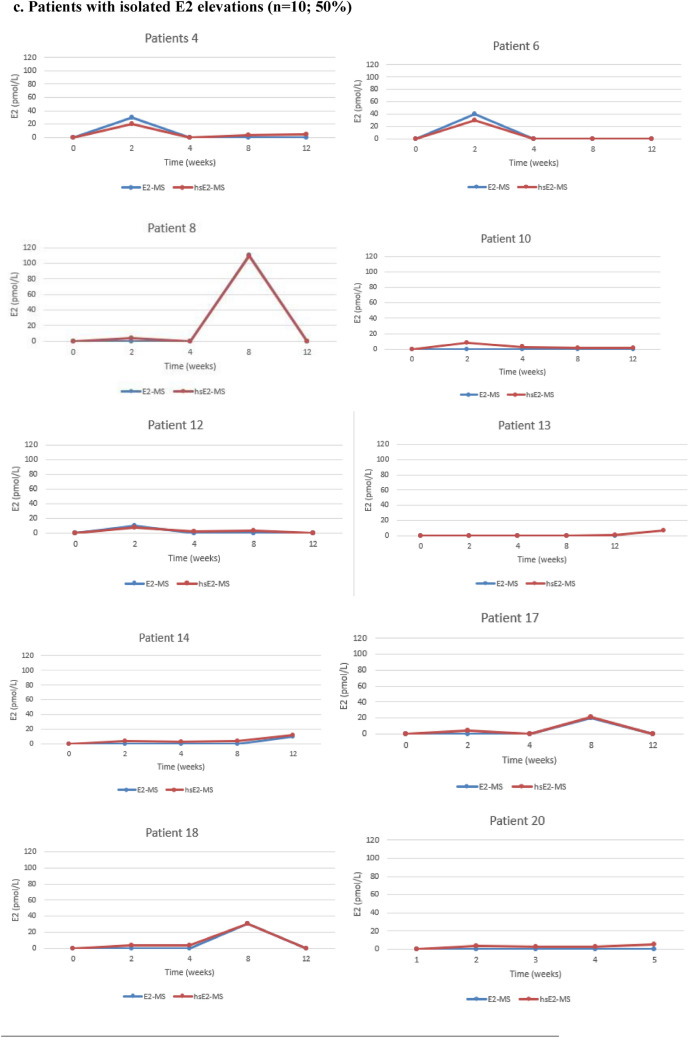
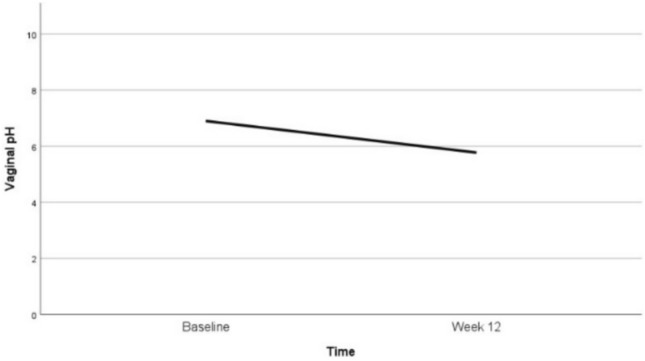
Results: At baseline, serum E2 levels, measured with hsE2-MS, were below the lower limit of quantification (LLOQ) in all patients. E2 remained below LLOQ throughout the treatment period in three patients (15%). Persistent E2 elevation above LLOQ was observed in six patients (30%), while isolated E2 elevations occurred in 10 patients (50%). One patient experienced transient E2 elevation in two sporadic measurements. Serum E2 variations were shown by using both LC-MS/MS methods. Vaginal pH, vaginal maturation index (VMI), and VVA symptoms significantly improved during treatment.
Conclusion: Intravaginal estradiol therapy (10ug) during adjuvant letrozole resulted in transient increases in systemic E2 levels among early BC patients with VVA. Highly sensitive LC-MS/MS is a promising method for monitoring E2 levels during aromatase inhibitor (AI) therapy.
Keywords: Aromatase inhibitor; Breast cancer; Estradiol; Intravaginal estrogen therapy; Liquid chromatography tandem mass spectrometry; Vulvovaginal atrophy.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interests: The authors declare no relevant financial or non-financial conflicts of interest. Ethical approval: This study was performed in accordance with the principles of the Declaration of Helsinki. Approval was obtained from the Ethics committee of Helsinki University Hospital on April 20, 2020. The trial is registered in the Helsinki and Uusimaa Hospital District Clinical Trials Register (EudraCT Number 2019–001234-34). Consent to participate: Informed consent was obtained from all participants included in this study. Consent to publication: The authors confirm that this manuscript does not contain any individual person’s data in any form.
Figures



Similar articles
-
Effects of letrozole on serum estradiol and estrone in postmenopausal breast cancer patients and tolerability of treatment: a prospective trial using a highly sensitive LC-MS/MS (liquid chromatography-tandem mass spectrometry) method for estrogen measurement.Breast Cancer Res Treat. 2023 Oct;201(3):425-435. doi: 10.1007/s10549-023-07054-3. Epub 2023 Jul 25. Breast Cancer Res Treat. 2023. PMID: 37491651 Free PMC article. Clinical Trial.
-
Vaginal Testosterone Cream vs Estradiol Vaginal Ring for Vaginal Dryness or Decreased Libido in Women Receiving Aromatase Inhibitors for Early-Stage Breast Cancer: A Randomized Clinical Trial.JAMA Oncol. 2017 Mar 1;3(3):313-319. doi: 10.1001/jamaoncol.2016.3904. JAMA Oncol. 2017. PMID: 27832260 Clinical Trial.
-
Monitoring serum estradiol levels in breast cancer patients during extended adjuvant letrozole treatment after five years of tamoxifen: a prospective trial.Breast Cancer Res Treat. 2021 Jun;187(3):769-775. doi: 10.1007/s10549-021-06168-w. Epub 2021 Mar 12. Breast Cancer Res Treat. 2021. PMID: 33710439 Clinical Trial.
-
Vaginal estrogen therapy in postmenopausal breast cancer patients treated with aromatase inhibitors.Arch Gynecol Obstet. 2012 May;285(5):1397-402. doi: 10.1007/s00404-011-2181-6. Epub 2012 Jan 3. Arch Gynecol Obstet. 2012. PMID: 22212649 Review.
-
Comparison of intravaginal 6.5mg (0.50%) prasterone, 0.3mg conjugated estrogens and 10μg estradiol on symptoms of vulvovaginal atrophy.J Steroid Biochem Mol Biol. 2017 Nov;174:1-8. doi: 10.1016/j.jsbmb.2017.03.014. Epub 2017 Mar 18. J Steroid Biochem Mol Biol. 2017. PMID: 28323042 Review.
References
-
- Burstein HJ, Lacchetti C, Anderson H, Buchholz TA, Davidson NE, Gelmon KA, Giordano SH, Hudis CA, Solky AJ, Stearns V et al (2019) Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: ASCO clinical practice guideline focused update. J Clin Oncol 37(5):423–438. 10.1200/JCO.18.01160 - PubMed
-
- Ganz PA, Rowland JH, Desmond K, Meyerowitz BE, Wyatt GE (1998) Life after breast cancer: understanding women’s health-related quality of life and sexual functioning. J Clin Oncol 16(2):501–514. 10.1200/jco.1998.16.2.501 - PubMed
-
- Cella D, Fallowfield LJ (2008) Recognition and management of treatment-related side effects for breast cancer patients receiving adjuvant endocrine therapy. Breast Cancer Res Treat 107(2):167–180. 10.1007/s10549-007-9548-1 - PubMed
-
- Chirgwin JH, Giobbie-Hurder A, Coates AS, Price KN, Ejlertsen B, Debled M, Gelber RD, Goldhirsch A, Smith I, Rabaglio M et al (2016) treatment adherence and its impact on disease-free survival in the breast international group 1–98 trial of tamoxifen and letrozole, alone and in sequence. J Clin Oncol 34(21):2452–2459. 10.1200/jco.2015.63.8619 - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
