

Hormone therapy enhances anti-PD1 efficacy in premenopausal estrogen receptor-positive and HER2-negative advanced breast cancer
- PMID: 39730000
- PMCID: PMC11866513
- DOI: 10.1016/j.xcrm.2024.101879
Hormone therapy enhances anti-PD1 efficacy in premenopausal estrogen receptor-positive and HER2-negative advanced breast cancer
Abstract
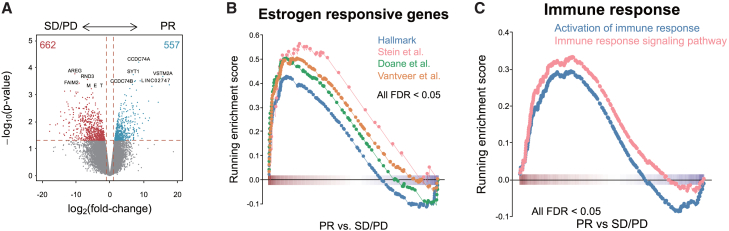
The efficacy of immunotherapy for estrogen receptor-positive/HER2-negative (ER+/HER2-) metastatic breast cancer (MBC) has not been proven. We conduct a phase 1b/2 trial to assess the efficacy of combining pembrolizumab (anti-PD1 antibody), exemestane (nonsteroidal aromatase inhibitor), and leuprolide (gonadotropin-releasing hormone agonist) for 15 patients with premenopausal ER+/HER2- MBC who had failed one to two lines of hormone therapy (HT) without chemotherapy. The primary endpoint of progression-free survival rate at 8 months (i.e., 64.3%) is achieved. Moreover, 5 of the 14 evaluable subjects exhibited partial responses (overall response rate = 35.7%). The combination of anti-PD1 antibody and anti-hormone therapy is associated with an enhanced immunoreactive microenvironment influencing treatment efficacy, as observed in pre- and post-treatment tumor samples through NanoString analysis. Post-treatment tumors are associated with increased immune response and immune cells. The findings indicate that combining HT with anti-PD1 antibody is a promising treatment strategy for patients with premenopausal ER+/HER2- MBC. This study was registered at ClinicalTrials.gov (NCT02990845).
Keywords: cancer; estrogen; estrogen suppression; gonadotropin-releasing hormone agonits; hormone therapy; immune cell infiltration; immunotherapy; luminal subtype; metastatic breast cancer; receptor positive/HER2 negative; tumor microenvironment.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests I.-C.C. received honoraria from AstraZeneca, Daiichi Sankyo, Gilead, Merck Sharp & Dohme, Novartis, Pfizer, and Sanofi and received research grants from AstraZeneca, Merck Sharp & Dohme, and Novartis. D.-Y.C. received honoraria from Amgen, AstraZeneca, Daiichi Sankyo, Eisai, Eli Lilly, MSD, Novartis, ONO Pharma, Pierre Faber, Pfizer, Roche, Sanofi, and TTY Biopharm. T.W.-W.C. received honoraria from Roche, Novartis, Eli Lilly, Eisai, Pfizer, Daiichi Sankyo, and AstraZeneca. Y.-S.L. received honoraria from Merck Sharp & Dohme and Pfizer and received research grants from Merck Sharp & Dohme and Pfizer.
Figures




References
-
- Mittendorf E.A., Zhang H., Barrios C.H., Saji S., Jung K.H., Hegg R., Koehler A., Sohn J., Iwata H., Telli M.L., et al. Neoadjuvant atezolizumab in combination with sequential nab-paclitaxel and anthracycline-based chemotherapy versus placebo and chemotherapy in patients with early-stage triple-negative breast cancer (IMpassion031): a randomised, double-blind, phase 3 trial. Lancet (London, England) 2020;396:1090–1100. doi: 10.1016/s0140-6736(20)31953-x. - DOI - PubMed
-
- Cortes J., Cescon D.W., Rugo H.S., Nowecki Z., Im S.A., Yusof M.M., Gallardo C., Lipatov O., Barrios C.H., Holgado E., et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): a randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet (London, England) 2020;396:1817–1828. doi: 10.1016/s0140-6736(20)32531-9. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
