

Mechanism of enhancing chemotherapy efficacy in pancreatic ductal adenocarcinoma with paricalcitol and hydroxychloroquine
- PMID: 39730001
- PMCID: PMC11866435
- DOI: 10.1016/j.xcrm.2024.101881
Mechanism of enhancing chemotherapy efficacy in pancreatic ductal adenocarcinoma with paricalcitol and hydroxychloroquine
Abstract
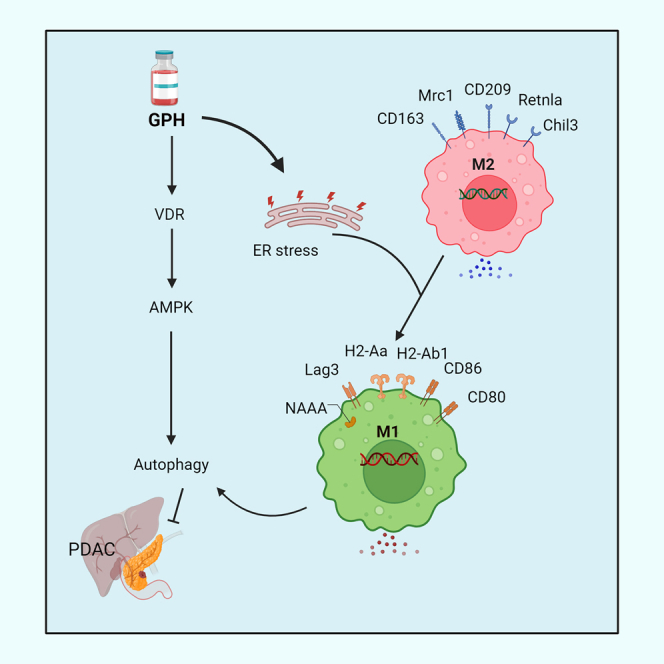
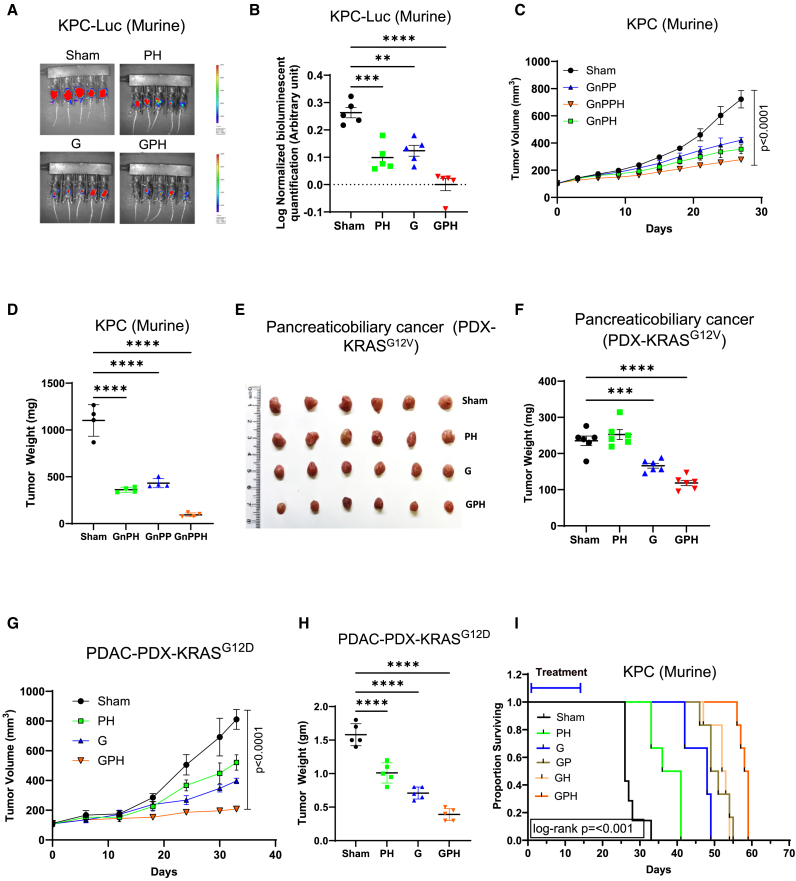
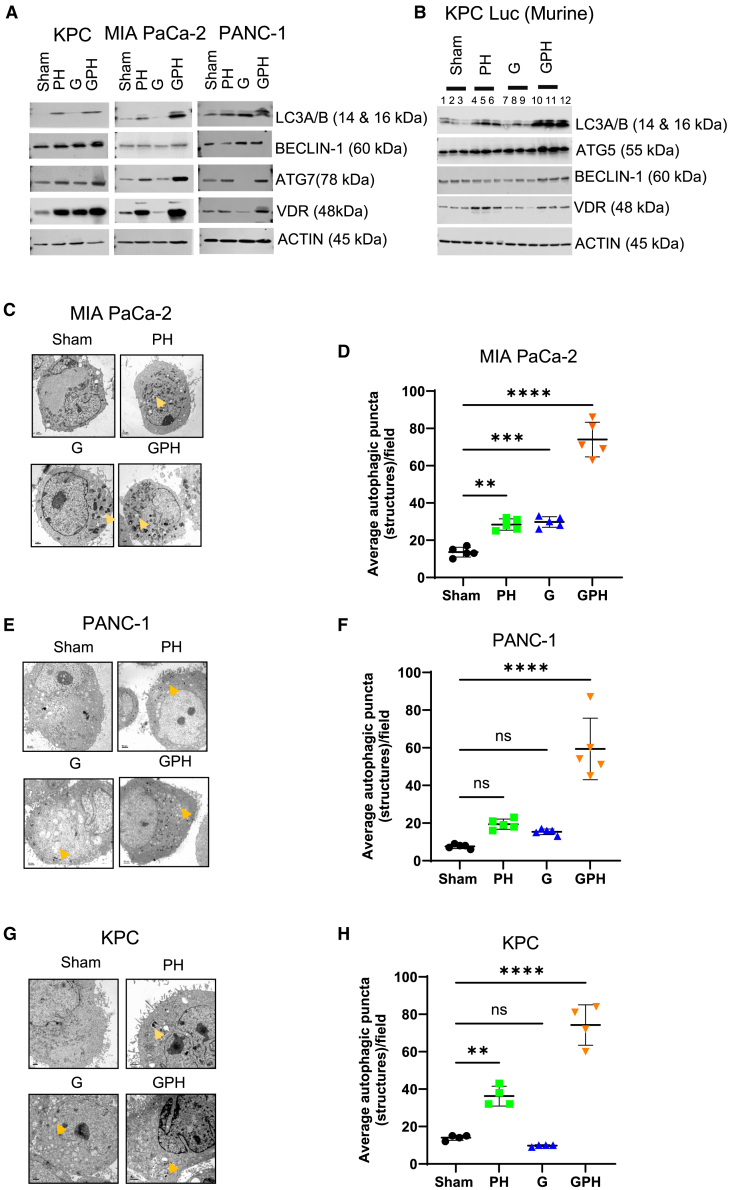
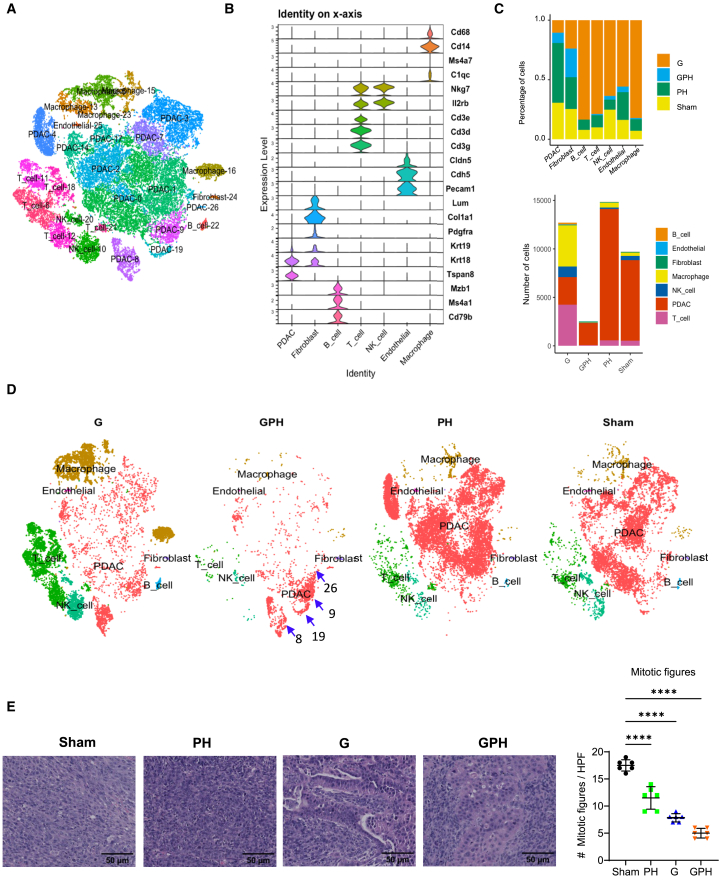
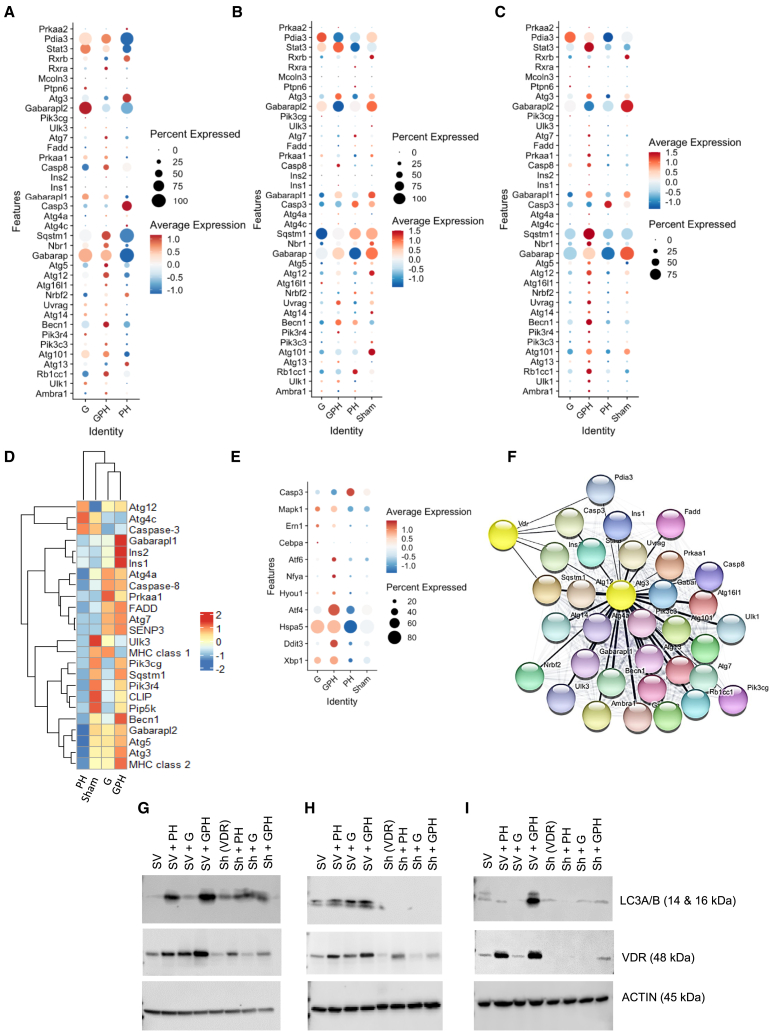
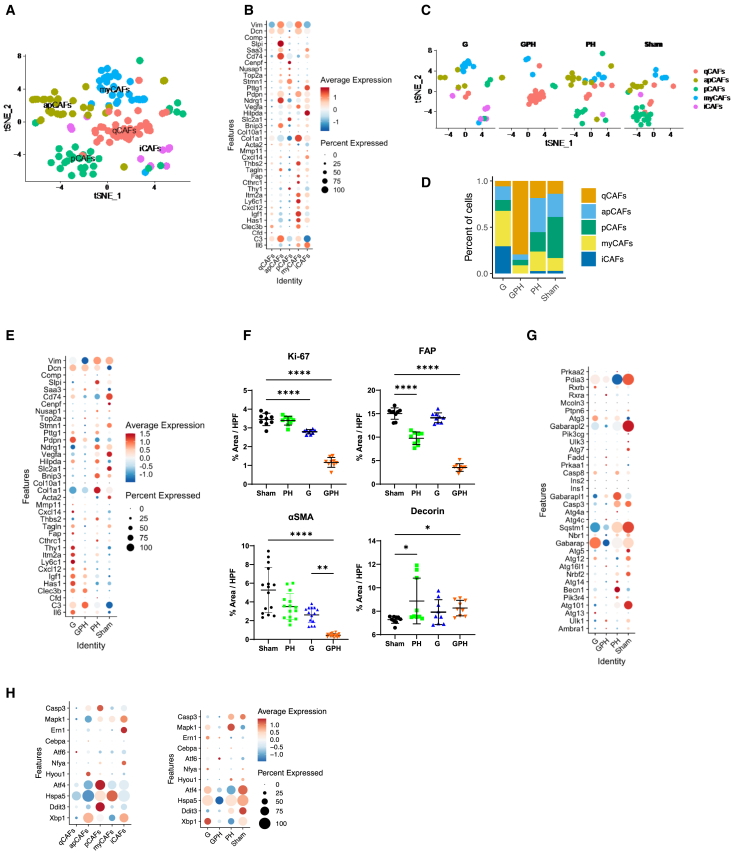
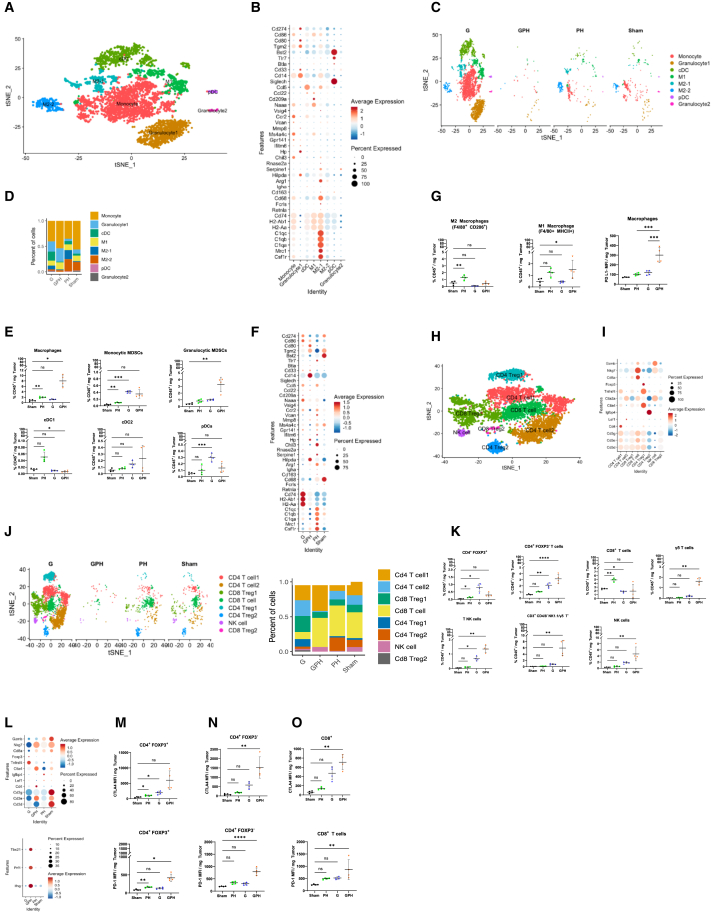
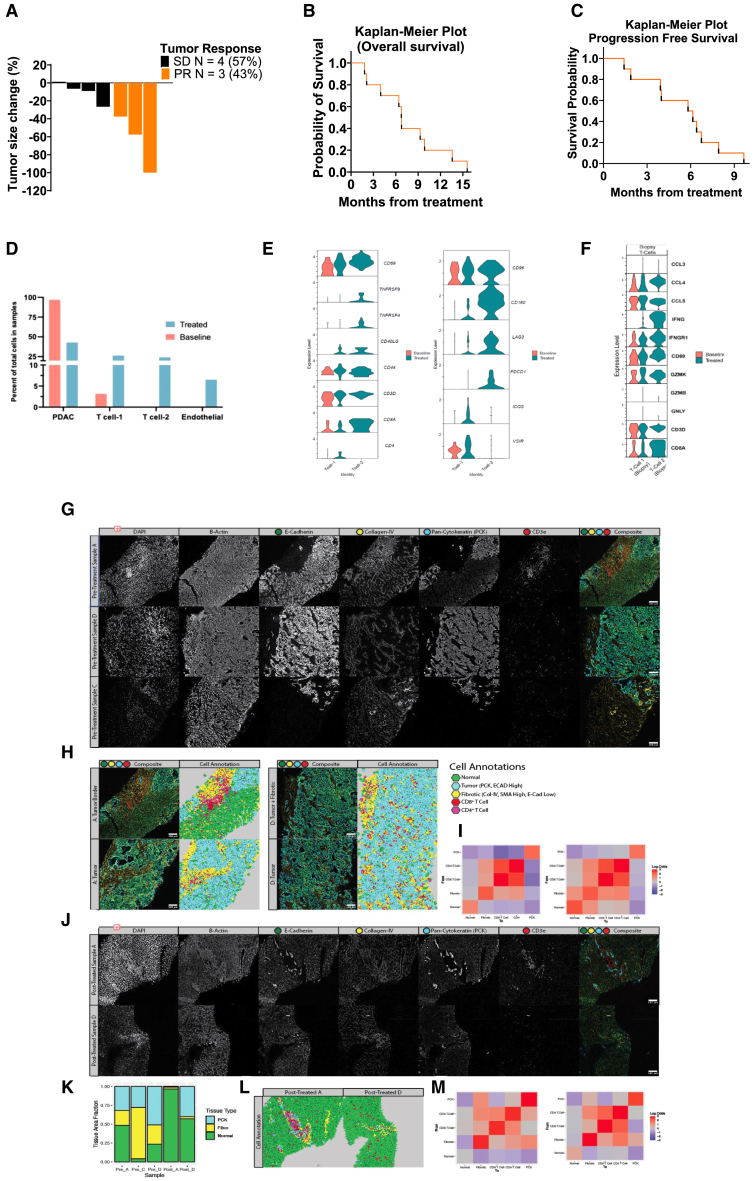
Pancreatic ductal adenocarcinoma (PDAC) has a minimal (<15%) 5-year existence, in part due to resistance to chemoradiotherapy. Previous research reveals the impact of paricalcitol (P) and hydroxychloroquine (H) on altering the lysosomal fusion, decreasing stromal burden, and triggering PDAC to chemotherapies. This investigation aims to elucidate the molecular properties of the H and P combination and their potential in sensitizing PDAC to gemcitabine (G). PH potentiates the effects of G in in vitro, orthotopic mouse models, and a patient-derived xenograft model of PDAC. Proteomic and single-cell RNA sequencing (RNA-seq) analyses reveal that GPH treatment upregulates autophagy and endoplasmic reticulum (ER) stress-related transcripts. GPH treatment decreases the number of Ki67, fibroblast-associated protein (FAP), and alpha-smooth muscle actin (SMA)-expressing fibroblasts with a decrease in autophagy-related transcripts. The GPH treatment increases M1 polarization and CD4+ and CD8+ T cells and reduces CD4+ and CD8+ regulatory T cells (Tregs). These effects of GPH were confirmed in paired biopsies obtained from patients treated in a clinical trial (NCT04524702).
Keywords: autophagy; cancer associated fibroblasts; chemotherapy; hydroxychloroquine; immune cells; pancreatic ductal adenocarcinoma; paricalcitol; proteomics; single-cell RNA-seq analyses; vitamin D receptor.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures
Similar articles
-
Paricalcitol plus hydroxychloroquine enhances gemcitabine activity and induces mesenchymal to epithelial transition in pancreatic ductal adenocarcinoma: A single cell RNA-seq analysis.Cancer Lett. 2025 Aug 10;625:217809. doi: 10.1016/j.canlet.2025.217809. Epub 2025 May 21. Cancer Lett. 2025. PMID: 40409452
-
Phosphorylation of USP32 by CDK5 regulates Rap1 stability and therapeutic resistance in pancreatic ductal adenocarcinoma.Oncogene. 2025 Aug;44(30):2634-2645. doi: 10.1038/s41388-024-03263-2. Epub 2025 May 16. Oncogene. 2025. PMID: 40379759
-
GPRC5A/CXCL8/NLRP3-mediated neutrophil extracellular traps drive gemcitabine-nab-paclitaxel resistance in pancreatic adenocarcinoma.Cancer Biol Med. 2025 Jul 15;22(7):832-53. doi: 10.20892/j.issn.2095-3941.2025.0040. Cancer Biol Med. 2025. PMID: 40665634 Free PMC article.
-
New Hope for Pancreatic Ductal Adenocarcinoma Treatment Targeting Endoplasmic Reticulum Stress Response: A Systematic Review.Int J Mol Sci. 2018 Aug 21;19(9):2468. doi: 10.3390/ijms19092468. Int J Mol Sci. 2018. PMID: 30134550 Free PMC article.
-
Chemotherapeutic agents eligible for prior dosing in pancreatic cancer patients requiring hemodialysis: a systematic review .Clin Nephrol. 2018 Aug;90(2):125-141. doi: 10.5414/CN109327. Clin Nephrol. 2018. PMID: 29578402
Cited by
-
The Role of the Tumor Microenvironment in Pancreatic Ductal Adenocarcinoma: Recent Advancements and Emerging Therapeutic Strategies.Cancers (Basel). 2025 May 8;17(10):1599. doi: 10.3390/cancers17101599. Cancers (Basel). 2025. PMID: 40427098 Free PMC article. Review.
-
Paricalcitol and hydroxychloroquine modulates extracellular matrix and enhance chemotherapy efficacy in pancreatic cancer.Res Sq [Preprint]. 2025 May 5:rs.3.rs-6406693. doi: 10.21203/rs.3.rs-6406693/v1. Res Sq. 2025. PMID: 40386428 Free PMC article. Preprint.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
