

A comprehensive review of massive transfusion and major hemorrhage protocols: origins, core principles and practical implementation
- PMID: 39730103
- PMCID: PMC11808514
- DOI: 10.1016/j.bjane.2024.844583
A comprehensive review of massive transfusion and major hemorrhage protocols: origins, core principles and practical implementation
Abstract
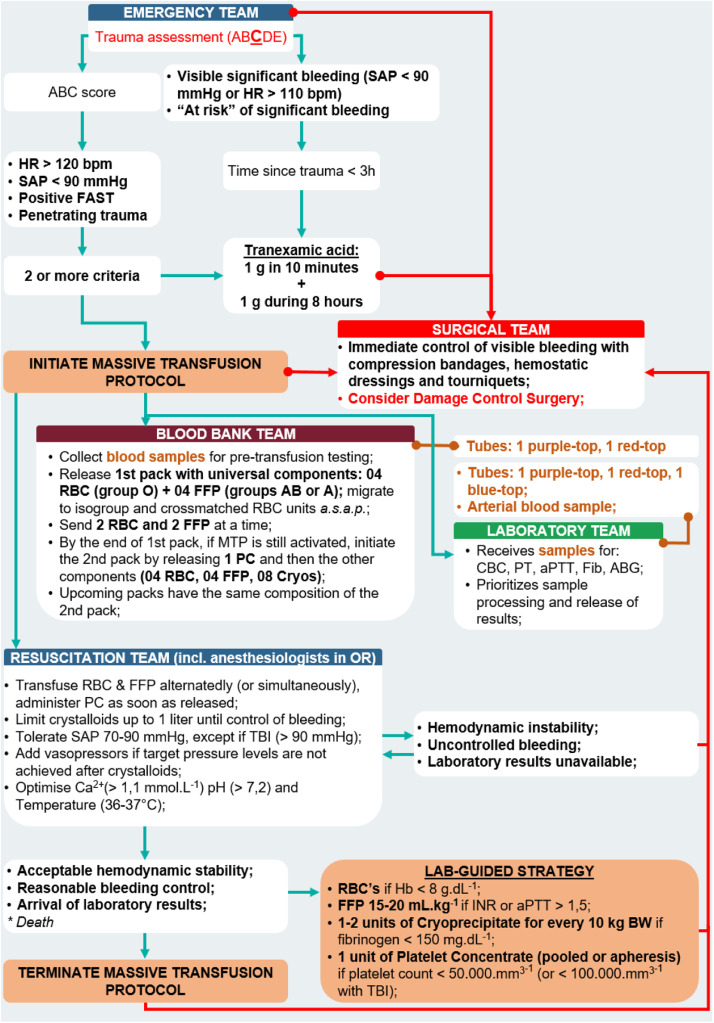
Until the beginning of the century, bleeding management was similar in elective surgeries or exsanguination scenarios: clotting tests were used to guide blood product orders and, while awaiting these results, an aggressive resuscitation with crystalloids was recommended. The high mortality rate in severe hemorrhages managed with this strategy endorsed the need for a special resuscitation plan. As a result, modifications were recommended to develop a new clinical approach to these patients, called "Damage Control Resuscitation". This strategy includes four principles: damage control surgery, minimization of crystalloids, permissive hypotension and hemostatic resuscitation. The latter involves the use of antifibrinolytics, correction of preconditions of hemostasis (calcium, pH and temperature) and the early and rapid restoration of intravascular volume with blood products. To enable timely availability and transfusion of blood products, specific actions in different hospital areas need to be synchronized, which are usually organized through Massive Transfusion Protocols or, as they have recently been rebranded, Major Hemorrhage Protocols (MHPs). Although these bundles of actions represent a paradigm change, essential aspects such as their historical evolution, theoretical foundations, terminology and operational elements have yet to be well explored. Considering the wide application range of these tools (emergency departments, interventional radiology, operating rooms and military fields), it is essential to integrate all professionals involved with severe hemorrhage scenarios in the implementation of the aforementioned protocols, from conception to execution and management. This review paper addresses MHP aspects relevant to anesthesiologists, transfusion services and other areas involved with the care of patients with severe bleeding.
Keywords: Blood coagulation disorders; Blood component transfusion; Exsanguination; Hemorrhage; Hemostasis; Shock, hemorrhagic.
Copyright © 2024. Published by Elsevier España S.L.U.
Conflict of interest statement
Conflicts of interest The authors declare no conflicts of interest.
Figures



References
-
- Eastridge BJ, Holcomb JB, Shackelford S. Outcomes of traumatic hemorrhagic shock and the epidemiology of preventable death from injury. Transfusion (Paris) 2019;59:1423–1428. - PubMed
-
- Armand R, Hess JR. Treating coagulopathy in trauma patients. Transfus Med Rev. 2003;17:223–231. - PubMed
-
- Holcomb JB, Jenkins D, Rhee P, et al. Damage control resuscitation: directly addressing the early coagulopathy of trauma. J Trauma. 2007;62:307–310. - PubMed
-
- Como JJ, Dutton RP, Scalea TM, Edelman BB, Hess JR. Blood transfusion rates in the care of acute trauma. Transfusion (Paris) 2004;44:809–813. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
