

Predictive modelling of hospital-acquired infection in acute ischemic stroke using machine learning
- PMID: 39730788
- PMCID: PMC11680783
- DOI: 10.1038/s41598-024-82280-3
Predictive modelling of hospital-acquired infection in acute ischemic stroke using machine learning
Abstract
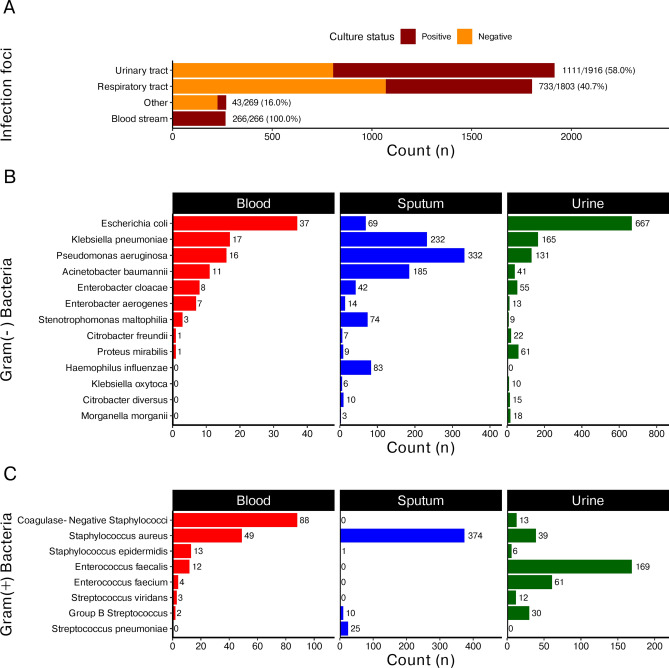
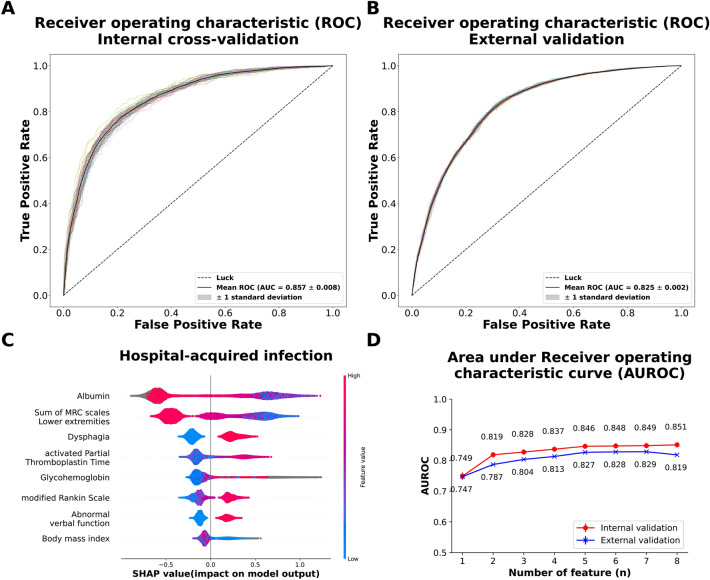
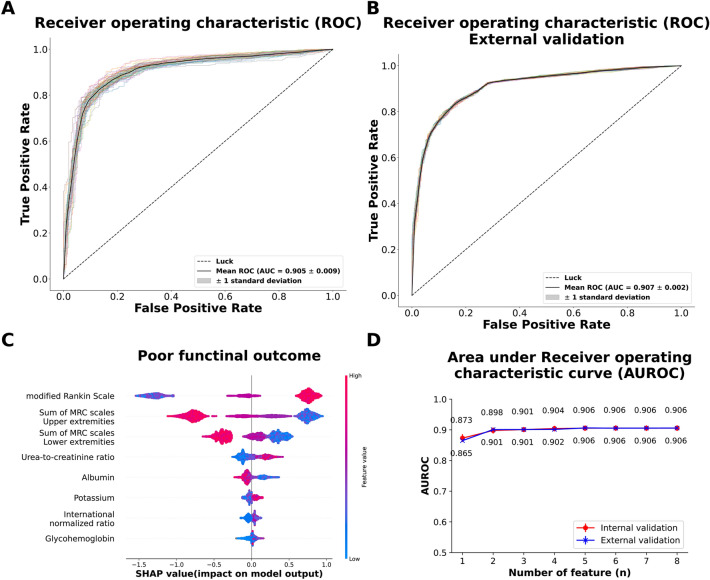
Hospital-acquired infections (HAIs) are serious complication for patients with acute ischemic stroke (AIS), often resulting in poor functional outcomes. However, no existing model can specifically predict HAI in AIS patients. Therefore, we employed the Gradient Boosting matching learning algorithm to establish predictive models for HAI occurrence in AIS patients and poor 30-day functional outcomes (modified Rankin Scale > 2) in AIS patients with HAI by analyzing electronic health records from 6560 AIS patients. Model performance was evaluated through internal cross-validation and external validation using an independent cohort of 3521 AIS patients. The established models demonstrated robust predictive performance for HAI in AIS patients, achieving area under the receiver operating characteristic curves (AUROCs) of 0.857 ± 0.008 during internal validation and 0.825 ± 0.002 during external validation. For AIS patients with HAI, the second model effectively predict poor 30-day functional outcomes, with AUROCs of 0.905 ± 0.009 during internal validation and 0.907 ± 0.002 during external validation. In conclusion, machine learning models effectively identify the HAI occurrence and predict poor 30-day functional outcomes in AIS patients with HAI. Future prospective studies are crucial for validating and refining these models for clinical application, as well as for developing an accessible flowchart or scoring system to enhance clinical practices.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
