

Smoking-associated electrocardiographic abnormalities predict cardiovascular mortality
- PMID: 39730843
- PMCID: PMC11680829
- DOI: 10.1038/s41598-024-82503-7
Smoking-associated electrocardiographic abnormalities predict cardiovascular mortality
Abstract
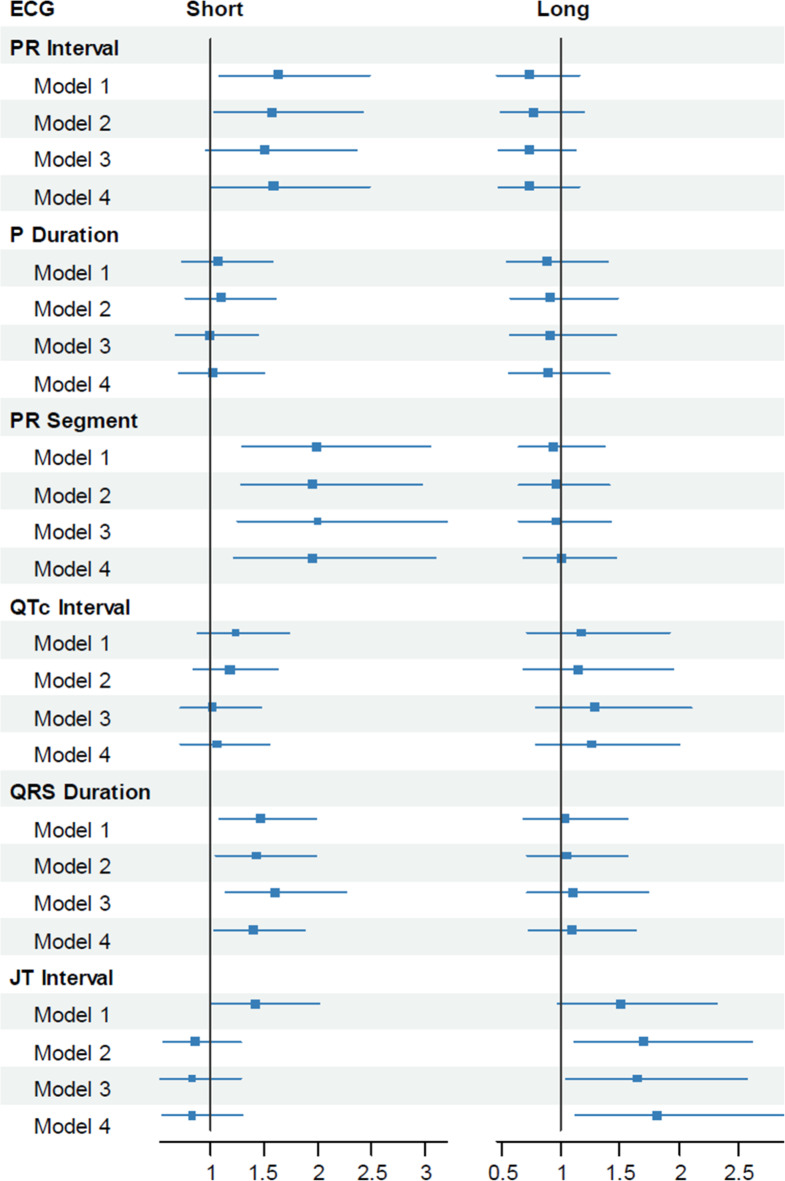
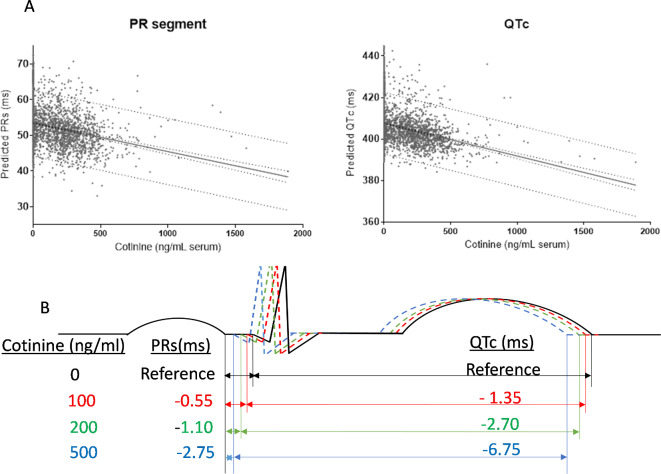
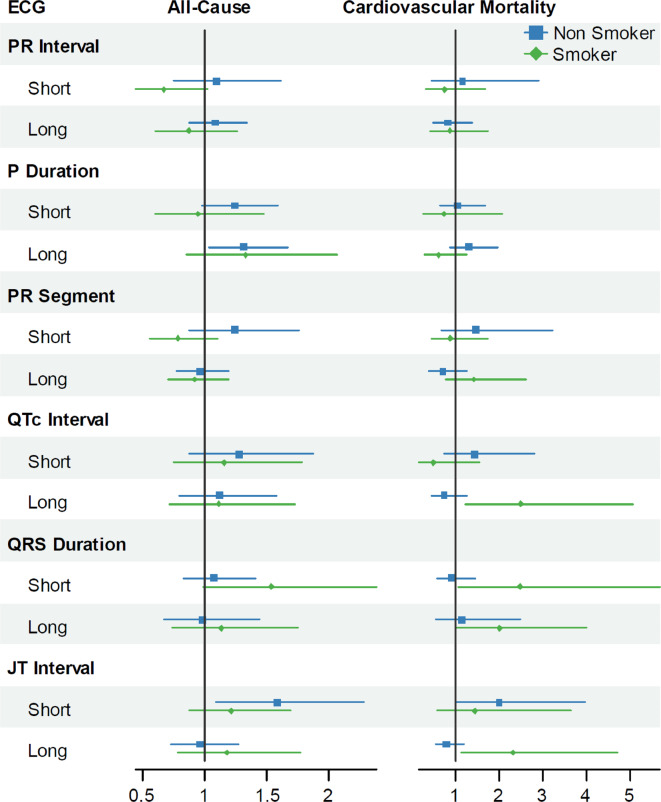
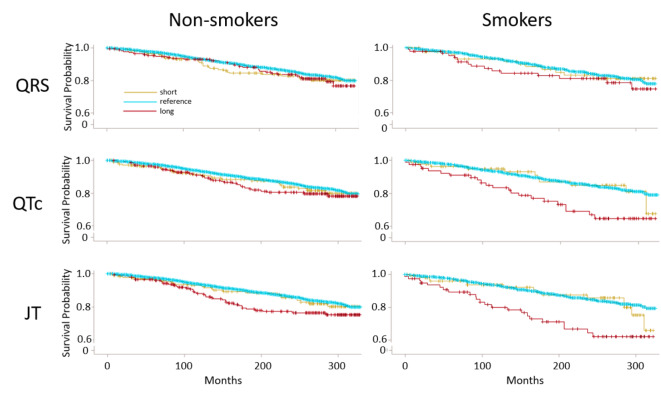
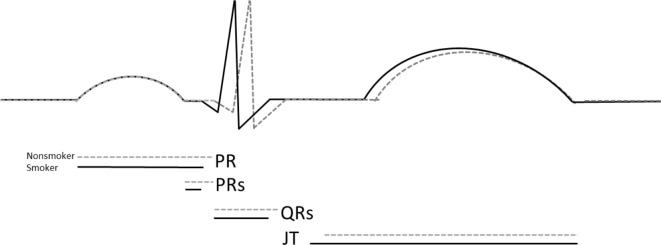
Background -Smoking is associated with arrhythmia and sudden cardiac death, but the biological mechanisms remain unclear. In electrocardiogram (ECG) recordings abnormal durations of ventricular repolarization (QT interval), atrial depolarization (P wave), and atrioventricular depolarization (PR interval and segment), predict cardiac arrhythmia and mortality. Previous analyses of the National Health and Nutrition Examination Survey (NHANES) database for associations between smoking and ECG abnormalities were incomplete. To elucidate how smoking affects cardiac excitation, we assessed in a nationally representative sample (NHANES III) the association between serum cotinine and P duration, PR interval, PR segment, rate-corrected QT (QTc), QRS duration, and JT interval. Methods and Results-We analyzed data from 5,653 adults using survey-weighted multinomial logistic regression to estimate associations between tobacco use (> 15 ng/ml serum cotinine) and short (< 5th percentile) or long (> 95th percentile) ECG intervals, relative to reference (5-95th percentile). After adjustment for demographics, risk factors, and conduction-altering medications, smoking was associated with a higher odds of short PR interval, PR segment, and QRS, and long JT. Broader effects of smoking on ECG were also assessed by survey-weighted linear regression of continuous cotinine and ECG, which revealed cotinine inversely associated with PR segment and QTc. Over a 22-year follow-up, many ECG abnormalities predicted cardiovascular mortality in smokers, including long JT, QRS, and QTc, and short QRS, whereas only short JT predicted mortality in nonsmokers. Conclusions -Smoking increases likelihood for rapid atrioventricular and ventricular depolarization and slow ventricular repolarization, which may promote cardiac arrhythmia and mortality.
Keywords: Cigarette; Cotinine; Electrocardiography; JT interval; P wave; PR interval; PR segment; QRS duration; QT interval; Smoking.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
Update of
-
Smoking-associated Electrocardiographic Abnormalities Predict Cardiovascular Mortality: Insights from NHANES.Res Sq [Preprint]. 2024 Jan 1:rs.3.rs-3615687. doi: 10.21203/rs.3.rs-3615687/v1. Res Sq. 2024. Update in: Sci Rep. 2024 Dec 28;14(1):31189. doi: 10.1038/s41598-024-82503-7. PMID: 38260619 Free PMC article. Updated. Preprint.
Similar articles
-
Smoking-associated Electrocardiographic Abnormalities Predict Cardiovascular Mortality: Insights from NHANES.Res Sq [Preprint]. 2024 Jan 1:rs.3.rs-3615687. doi: 10.21203/rs.3.rs-3615687/v1. Res Sq. 2024. Update in: Sci Rep. 2024 Dec 28;14(1):31189. doi: 10.1038/s41598-024-82503-7. PMID: 38260619 Free PMC article. Updated. Preprint.
-
Smoking Accelerates Atrioventricular Conduction in Humans Concordant with Increased Dopamine Release.Cardiovasc Toxicol. 2021 Feb;21(2):169-178. doi: 10.1007/s12012-020-09610-5. Epub 2020 Oct 12. Cardiovasc Toxicol. 2021. PMID: 33043409 Free PMC article.
-
Risk of Mortality Associated With QT and JT Intervals at Different Levels of QRS Duration (from the Third National Health and Nutrition Examination Survey).Am J Cardiol. 2015 Jul 1;116(1):74-8. doi: 10.1016/j.amjcard.2015.03.038. Epub 2015 Apr 6. Am J Cardiol. 2015. PMID: 25929581 Free PMC article.
-
Electrocardiographic conduction and repolarization markers associated with sudden cardiac death: moving along the electrocardiography waveform.Minerva Cardioangiol. 2019 Apr;67(2):131-144. doi: 10.23736/S0026-4725.18.04775-8. Epub 2018 Sep 26. Minerva Cardioangiol. 2019. PMID: 30260143 Review.
-
Assessment of QTc and Risk of Torsades de Pointes in Ventricular Conduction Delay and Pacing: A Review of the Literature and Call to Action.J Acad Consult Liaison Psychiatry. 2021 Sep-Oct;62(5):501-510. doi: 10.1016/j.jaclp.2021.02.003. Epub 2021 Feb 13. J Acad Consult Liaison Psychiatry. 2021. PMID: 34489062 Review.
Cited by
-
Acute and Persistent Cardiovascular Effects of Menthol E-Cigarettes in Mice.J Am Heart Assoc. 2025 May 6;14(9):e037420. doi: 10.1161/JAHA.124.037420. Epub 2025 Apr 25. J Am Heart Assoc. 2025. PMID: 40281649 Free PMC article.
References
-
- 1. Centers for Disease C, Prevention. Smoking-attributable mortality, years of potential life lost, and productivity losses–United States, 2000–2004. MMWR Morb Mortal Wkly Rep. 2008;57:1226–1228. - PubMed
-
- 4. Dai H, Zhang Q, Much AA, Maor E, Segev A, Beinart R, Adawi S, Lu Y, Bragazzi NL, Wu J. Global, regional, and national prevalence, incidence, mortality, and risk factors for atrial fibrillation, 1990–2017: results from the Global Burden of Disease Study 2017. Eur Heart J Qual Care Clin Outcomes. 2021;7:574–582. doi: 10.1093/ehjqcco/qcaa061 - PMC - PubMed
-
- 5. Aune D, Schlesinger S, Norat T, Riboli E. Tobacco smoking and the risk of atrial fibrillation: A systematic review and meta-analysis of prospective studies. Eur J Prev Cardiol. 2018;25:1437–1451. doi: 10.1177/2047487318780435 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
