

Multiomics integration and machine learning reveal prognostic programmed cell death signatures in gastric cancer
- PMID: 39730893
- PMCID: PMC11680692
- DOI: 10.1038/s41598-024-82233-w
Multiomics integration and machine learning reveal prognostic programmed cell death signatures in gastric cancer
Abstract
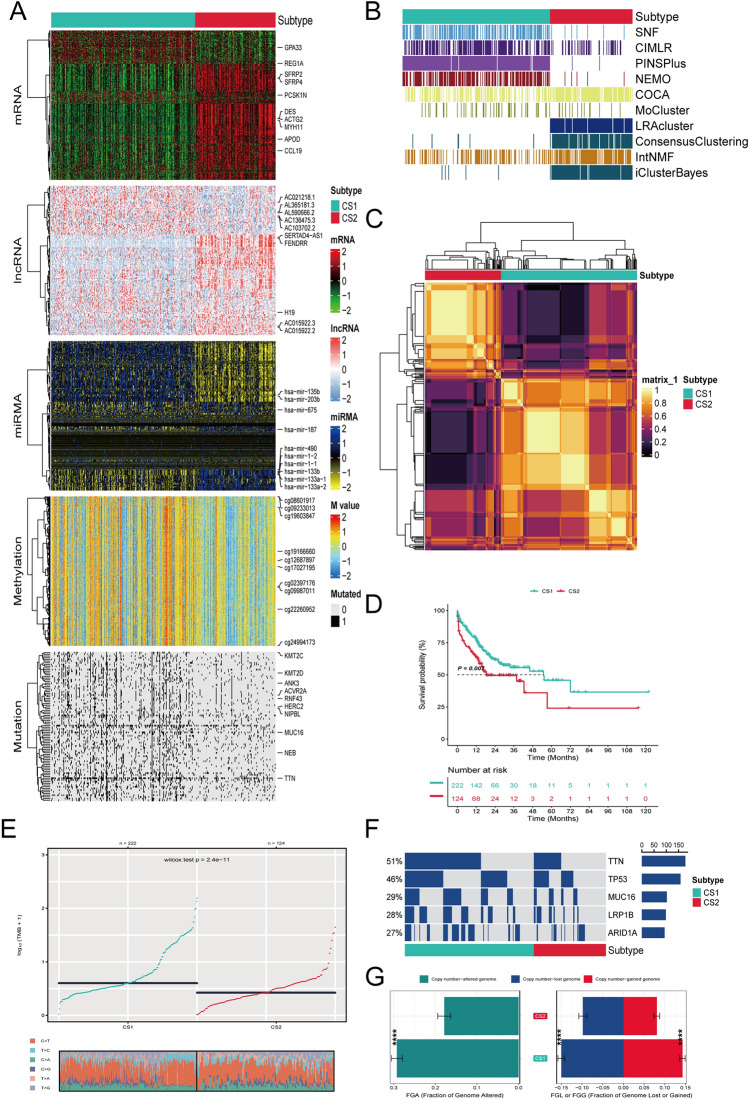
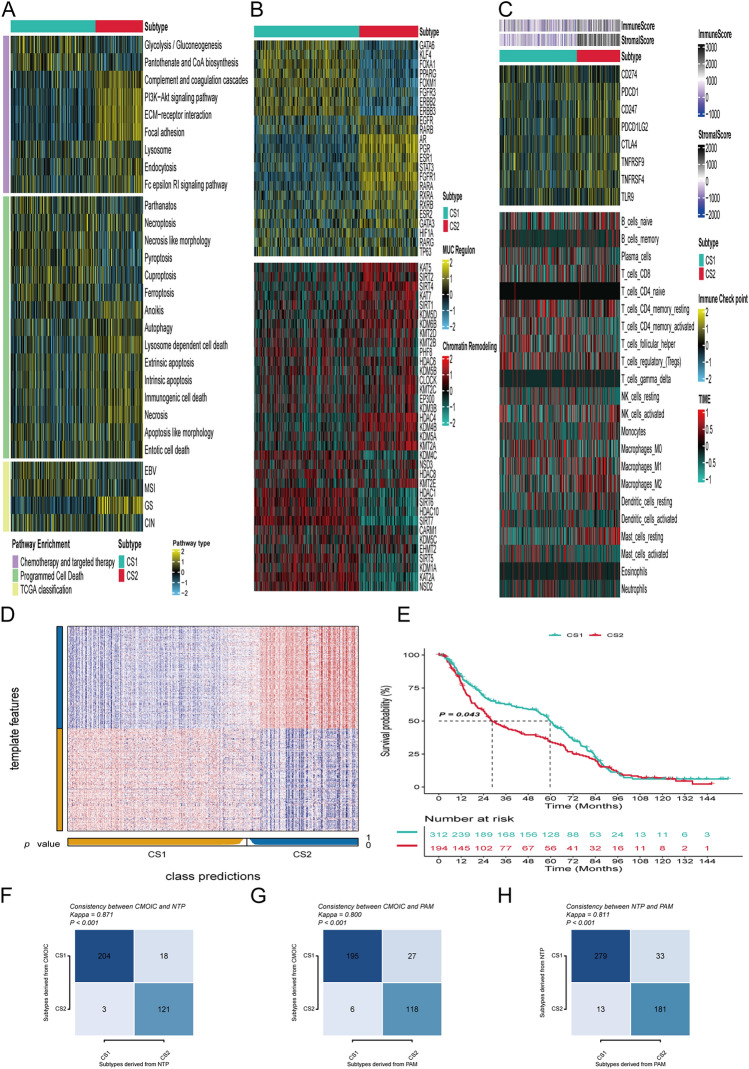
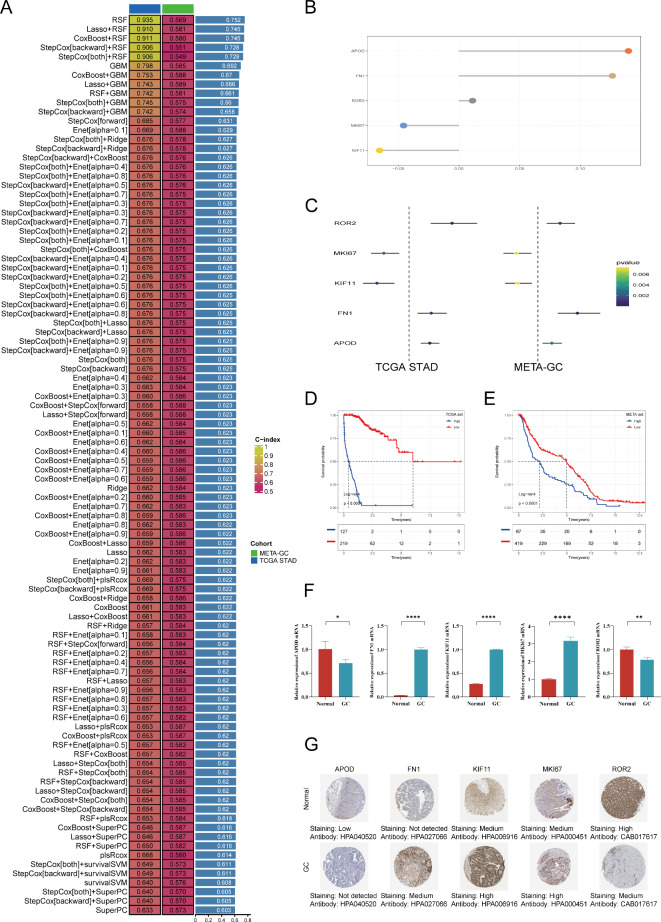
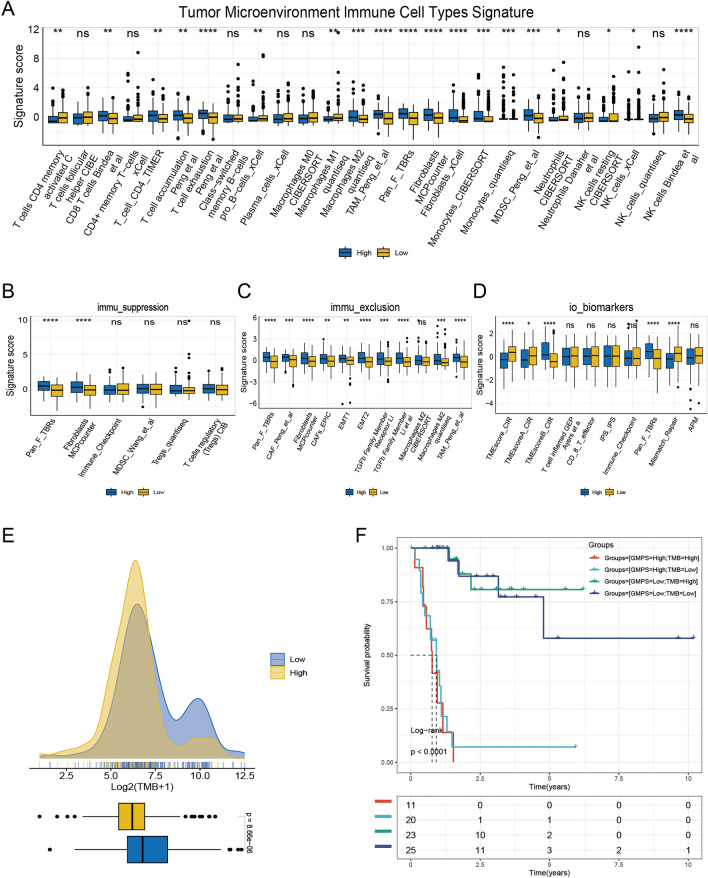
Gastric cancer (GC) is characterized by notable heterogeneity and the impact of molecular subtypes on treatment and prognosis. The role of programmed cell death (PCD) in cellular processes is critical, yet its specific function in GC is underexplored. This study applied multiomics approaches, integrating transcriptomic, epigenetic, and somatic mutation data, with consensus clustering algorithms to classify GC molecular subtypes and assess their biological and immunological features. A machine learning model was developed to create the Gastric Cancer Multi-Omics Programmed Cell Death Signature (GMPS), targeting PCD-related genes. We verified the expression of the GMPS hub genes using the RT-qPCR method. The prognostic influence of GMPS on GC was then evaluated. Single-cell analysis was performed to examine the heterogeneity of PCD characteristics in GC. Findings indicate that GMPS notably correlates with patient survival rates, tumor mutational burden (TMB), and copy number variations (CNV), demonstrating substantial prognostic predictive power. Moreover, GMPS is closely associated with the tumor microenvironment (TME) and immune therapy response. This research elucidates the molecular subtypes of GC, highlighting PCD's critical role in prognosis assessment. The relationship between GMPS and immune therapy response, alongside gastric cancer's microenvironmental features, provides insights for personalized treatment.
Keywords: Gastric cancer; Machine learning; Multiomics; Prognosis; Programmed cell death.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
