

The correlation between Fischer's ratio and the risk of cardiac dysfunction in heart failure patients
- PMID: 39731046
- PMCID: PMC11681758
- DOI: 10.1186/s12872-024-04433-6
The correlation between Fischer's ratio and the risk of cardiac dysfunction in heart failure patients
Abstract
Backgrounds: Due to the high mortality and hospitalization rate in chronic heart failure (HF), it is of great significance to study myocardial nutrition conditions. Amino acids (AAs) are essential nutrient metabolites for cell development and survival. This study aims to investigate the associations and prognostic value of plasma branched-chain amino acid/aromatic amino acid ratio (Fischer's ratio, FR) in patients with left ventricular ejection fraction (LVEF) ≤ 50%.
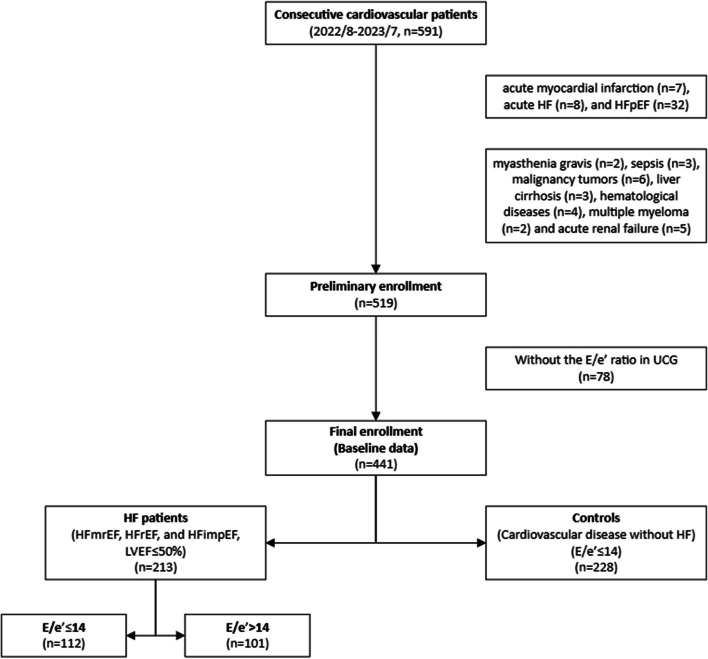
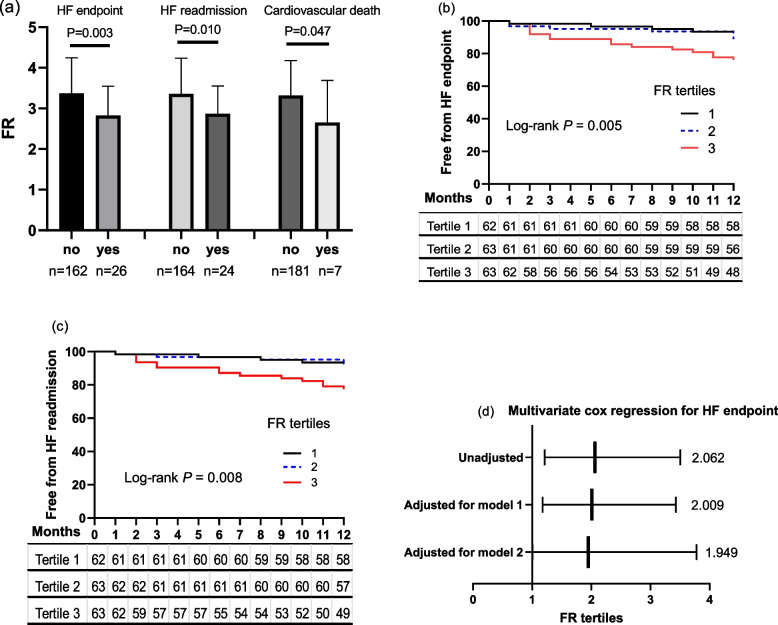
Methods: The value of serum AAs was obtained from 441 cardiovascular patients by liquid chromatography-tandem, including 213 HF patients [all LVEF ≤ 50%, E/e'>14 (n = 101) and E/e'≤14 (n = 112)], and 228 controls without HF [(excluding HF with preserved ejection fraction (EF)]. Two-dimensional echocardiography and Doppler flow imaging determined LVEF and the ratio of early diastolic mitral inflow to mitral annular tissue velocities (E/e'). The abnormal LVEF (≤ 50%) refers to the definition of HF with reduced, mildly reduced, or improved EF. The logistic regression analysis was conducted to measure the FR index and the risk of cardiac dysfunction, and further confirmed by receiver-operating characteristic curves (ROC curve) analysis. In the prospective study, the 188 HF patients were followed up for a mean year (11.74 ± 1.44 months). The event-free HF endpoint or HF readmission was determined by Kaplan-Meier curves, and differences were assessed using log-rank tests, respectively. Cox regression analysis was used to further assess the prognostic value of FR in HF.
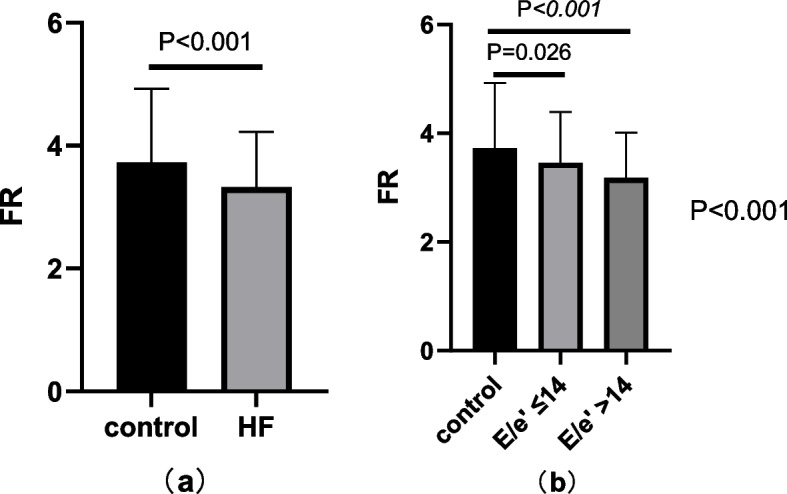
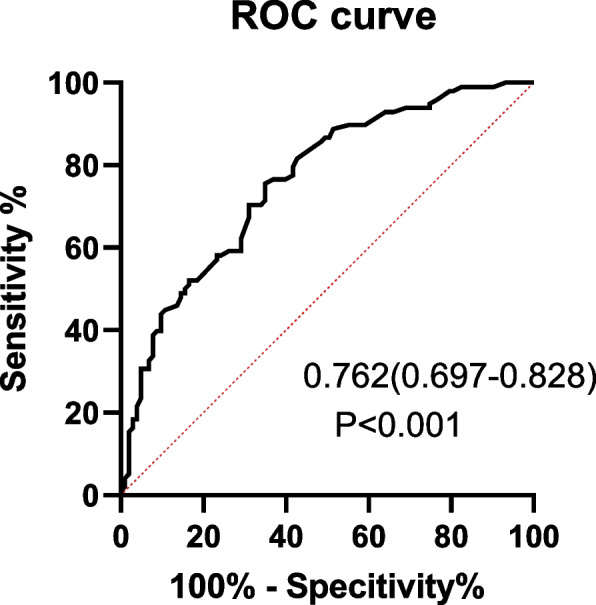
Results: FR index decreased gradually along with the control group, HF with E/e'≤14 group, and HF with E/e'>14 group (3.73 ± 1.20 vs. 3.45 ± 0.94 vs. 3.18 ± 0.83, respectively, P < 0.001). Low FR index was associated with HF after full adjustment in all patients [odds ratio (OR): 2.072; 95% confidence interval (CI): 1.546-2.776; P < 0.001]. Meanwhile, low FR index was the independent risk factor for E/e'>14 in HF patients (OR:1.659; 95% CI:1.125-2.446; P = 0.011). The area under the ROC curve for predicting abnormal E/e' was 0.762 (sensitivity 75.51%, specificity 65.05%) by multivariate logistic regression. Furthermore, the decreased FR values indicated poor HF endpoint or HF readmission in HF patients (all Log-rank P < 0.01). The Cox regression analysis showed that low FR tertiles remained correlated to the risk of HF endpoint [hazard ratio (HR): 1.949; 95% CI: 1.006-3.778; P = 0.048].
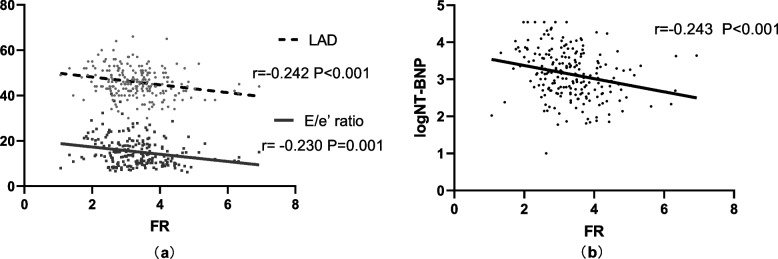
Conclusions: In all patients, low FR confers an increased risk for predicting HF. Decreased FR levels could also indicate increased left ventricular (LV) filling pressure in HF. In addition, a lower FR value was associated with higher HF endpoint events. Thus, FR can be a valuable indicator of heart function.
Keywords: Cardiac dysfunction; Chronic heart failure; LV filling pressure; Low fischer’s ratio; Prognosis; Risk prediction.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study followed the principles outlined in the Declaration of Helsinki. The study protocol was approved by the Ethics committee of Rui Jin Hospital, Shanghai Jiao Tong University School of Medicine (2016-019, Exploring the clinical status and prognostic factors of patients with chronic heart failure). Written informed consent was obtained from all participants. Consent for publication: There are no details on individuals within the manuscript. Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Ambrosy AP, Fonarow GC, Butler J, Chioncel O, Greene SJ, Vaduganathan M, Nodari S, Lam CSP, Sato N, Shah AN, Gheorghiade M. The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J Am Coll Cardiol. 2014;63(12):1123–33. - PubMed
-
- Mentz RJ, O’Connor CM. Pathophysiology and clinical evaluation of acute heart failure. Nat Rev Cardiol. 2016;13(1):28–35. - PubMed
-
- Solomon SD, Anavekar N, Skali H, McMurray JJ, Swedberg K, Yusuf S, Granger CB, Michelson EL, Wang D, Pocock S, Pfeffer MA. Candesartan in Heart failure reduction in mortality (CHARM) investigators. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation. 2005;112:3738–44. - PubMed
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson LW, Vardeny O, Vest AR, Yancy CW. 2022 AHA/ACC/HFSA Guideline for the management of Heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice guidelines. Circulation. 2022;145:e895–1032. - PubMed
-
- DiNicolantonio JJ, Liu J, O’Keefe JH. Thiamine and Cardiovascular Disease: A literature review. Prog Cardiovasc Dis. 2018;61(1):27–32. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
