

Combined immunohistochemistry of PRAME and p16 in the differentiation of melanocytic neoplasms, with a detailed focus on acral lesions
- PMID: 39731107
- PMCID: PMC11681745
- DOI: 10.1186/s13000-024-01586-y
Combined immunohistochemistry of PRAME and p16 in the differentiation of melanocytic neoplasms, with a detailed focus on acral lesions
Abstract
Background: Isolated immunohistochemical indicators are limited to diagnose melanocytic neoplasms. This retrospective study is to assess the diagnostic value of combined immunohistochemical analysis targeting preferentially expressed antigen in melanoma (PRAME) and p16 in melanocytic neoplasms, with a detailed focus on arcal lesions.
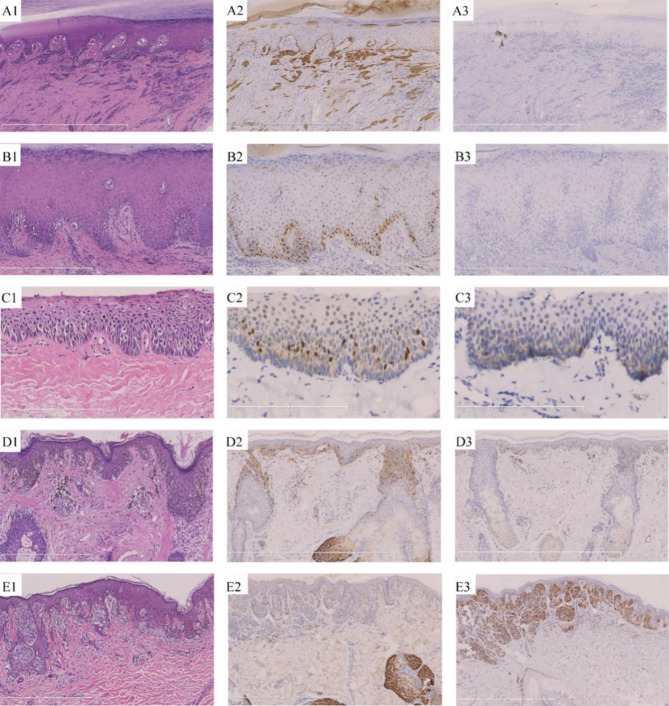
Methods: This was a single center cohort study from January 2022 to June 2023. A total of 165 identified cases were collected, including 112 melanomas (MMs) and 53 melanocytic nevi, which were composed of 122 acral samples and 43 non-acral samples. Immunohistochemistry(IHC) for both PRAME and p16 was performed in these cases, which was subsequently statistically analyzed to assess the diagnosis ability of PRAME and p16.
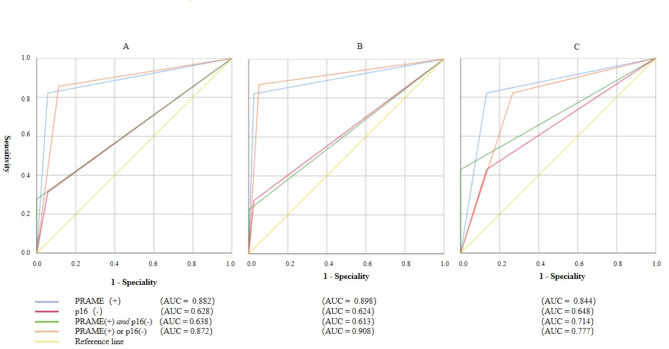
Results: In total samples, the sensitivity and specificity of PRAME(+) for MM are 82.1% and 94.3% (AUC = 0.882, 95%CI:0.827-0.938), while of p16(-) for MM are 31.25% and 94.3% (AUC = 0.628, 95%CI:0.542-0.714); PRAME(+)/p16(-) (meaning as PRAME(+) or p16(-)) displayed a sensitivity and specificity of 85.7% and 88.7% for MM (AUC = 0.872, 95%CI:0.810-0.934), while PRAME(+) &p16(-) (meaning as PRAME(+) and p16(-)) revealed a sensitivity and specificity of 27.7% and 100% in MM (AUC = 0.638, 95%CI:0.555-0.722). In acral samples, PRAME(+)/p16(-) exhibited a specificity of 94.7% and a sensitivity of 86.9% for MM (AUC = 0.908, 95%CI: 0.849-0.968), with sensitivities of 90.9% for invasive MM and 82.5% for preinvasive MM, respectively; The sensitivity and specificity of PRAME(+) &p16(-) for MM is 22.6% and 100% (AUC = 0.613, 95%CI: 0.513-0.714) respectively. In non-acral samples, the sensitivity and specificity of PRAME(+)/p16(-) for MM are 82.1% and 73.3% (AUC = 0.777, 95%CI: 0.622-0.933), while of PRAME(+) &p16(-) are 42.9% and 100% (AUC = 0.714, 95%CI:0.564-0.864).
Conclusion: Combined IHC of PRAME and p16 contributes to discriminating melanocytic neoplasms, especially for in situ acral MM.
Keywords: Immunohistochemistry(IHC); Melanocytic nevus; Melanoma (MM); PRAME; p16.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical clearance for the study was obtained from the Institutional Review Board of Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College (Ethical Approval: No. 2013-LC/KY-033). Moreover, written informed consent was conscientiously acquired from all patients or their legal guardians. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
