

Feasibility and safety of ultra-low volume ventilation (≤ 3 ml/kg) combined with extra corporeal carbon dioxide removal (ECCO2R) in acute respiratory failure patients
- PMID: 39731126
- PMCID: PMC11674201
- DOI: 10.1186/s13054-024-05168-8
Feasibility and safety of ultra-low volume ventilation (≤ 3 ml/kg) combined with extra corporeal carbon dioxide removal (ECCO2R) in acute respiratory failure patients
Abstract
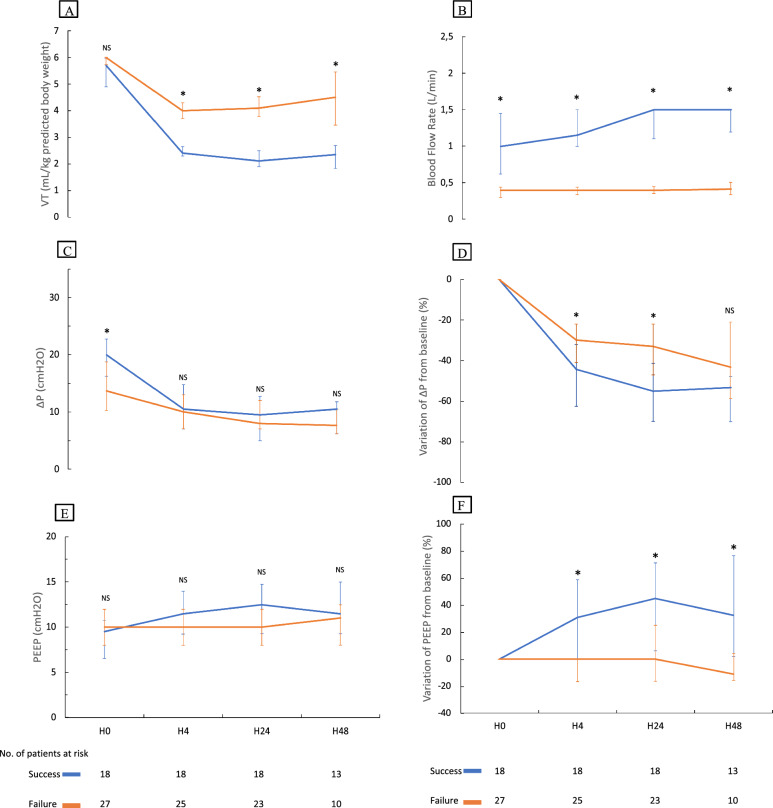
Background: Ultra-protective ventilation is the combination of low airway pressures and tidal volume (Vt) combined with extra corporeal carbon dioxide removal (ECCO2R). A recent large study showed no benefit of ultra-protective ventilation compared to standard ventilation in ARDS (Acute Respiratory Distress Syndrome) patients. However, the reduction in Vt failed to achieve the objective of less than or equal to 3 ml/kg predicted body weight (PBW). The main objective of our study was to assess the feasibility of the ultra-low volume ventilation (Vt ≤ 3 ml/kg PBW) facilitated by ECCO2R in acute respiratory failure patients.
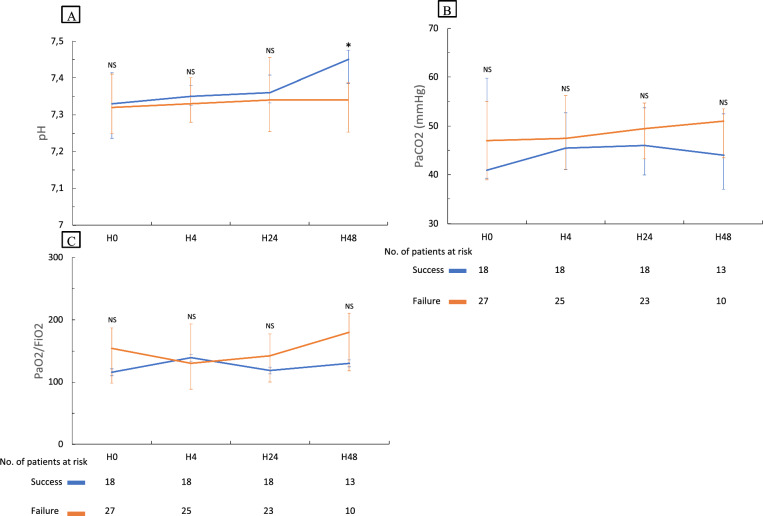
Methods: Retrospective analysis of a prospective cohort of patients with either high or low blood flow veno-venous ECCO2R devices. A session was defined as a treatment of ECCO2R from the start to the removal of the device (one patient could have one more than one session). Primary endpoint was the proportion of sessions during which a Vt less or equal to 3 ml/kg PBW at 24 h after the start of ECCO2R was successfully achieved for at least 12 h. Secondary endpoints were respiratory variables, rate of adverse events and outcomes.
Results: Forty-five ECCO2R sessions were recorded among 41 patients. Ultra-low volume ventilation (tidal volume ≤ 3 ml/kg PBW, success group) was successfully achieved at 24 h in 40.0% sessions (18 out of 45 sessions, confidence interval 25.3-54.6%). At 24 h, tidal volume in the failure group was 4.1 [3.8-4.5] ml/kg PBW compared to 2.1 [1.9-2.5] in the success group (p < 0.001). After multivariate analysis, blood flow rate was significantly associated with success of ultra-low volume ventilation (adjusted OR per 100 ml/min increase 1.51 (95%CI 1.21-1.90, p = 0.0003).
Conclusion: Ultra-low volume ventilation (≤ 3 ml/kg PBW) was feasible in 18 out of 45 sessions. Higher blood flow rates were associated with the success of ultra-low volume ventilation.
Keywords: Acute respiratory distress syndrome; ECCO2R; Extracorporeal carbon dioxide removal; Intensive care; Ventilator-induced lung injury.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The institutional ethics committee reviewed the retrospective use of anonymous data for scientific purpose and waived the need to obtain informed written consent. The Institutional Review Board (IRB) of Montpellier University Hospital approved the study (2019_IRB-MTP_05-25). Consent for publication: Not applicable. Competing interests: Pr Jaber reports receiving consulting fees from Drager, Medtronic, Mindray, Fresenius, Baxter, and Fisher & Paykel. Pr De Jong reports receiving remuneration for presentations from Medtronic, Drager and Fisher & Paykel. Dr Monet reports receiving remuneration for presentations from Medtronic. The other authors declare that they have no competing interests.
Figures
Comment in
-
Questioning the classification of "high blood flow" versus "low blood flow" ECCO₂R in ultra-low tidal volume ventilation studies: a call for functional classification.Crit Care. 2025 Mar 19;29(1):121. doi: 10.1186/s13054-025-05352-4. Crit Care. 2025. PMID: 40108676 Free PMC article. No abstract available.
-
"High blood flow" versus "low blood flow" ECCO2R: how to classify-author's reply.Crit Care. 2025 Apr 18;29(1):156. doi: 10.1186/s13054-025-05386-8. Crit Care. 2025. PMID: 40251692 Free PMC article. No abstract available.
References
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. - PubMed
-
- Behrendt CE. Acute respiratory failure in the United States: incidence and 31-day survival. Chest. 2000;118(4):1100–5. - PubMed
-
- Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. 2013;369(22):2126–36. - PubMed
-
- Tremblay LN, Slutsky AS. Ventilator-induced lung injury: from the bench to the bedside. Intensive Care Med. 2006;32(1):24–33. - PubMed
-
- Plötz FB, Slutsky AS, van Vught AJ, Heijnen CJ. Ventilator-induced lung injury and multiple system organ failure: a critical review of facts and hypotheses. Intensive Care Med. 2004;30(10):1865–72. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
