

Safety of baricitinib in vaccinated patients with severe and critical COVID-19 sub study of the randomised Bari-SolidAct trial
- PMID: 39731852
- PMCID: PMC11743795
- DOI: 10.1016/j.ebiom.2024.105511
Safety of baricitinib in vaccinated patients with severe and critical COVID-19 sub study of the randomised Bari-SolidAct trial
Abstract
Background: The Bari-SolidAct randomized controlled trial compared baricitinib with placebo in patients with severe COVID-19. A post hoc analysis revealed a higher incidence of serious adverse events (SAEs) among SARS-CoV-2-vaccinated participants who had received baricitinib. This sub-study aimed to investigate whether vaccination influences the safety profile of baricitinib in patients with severe COVID-19.
Methods: Biobanked samples from 146 participants (55 vaccinated vs. 91 unvaccinated) were analysed longitudinally for inflammation markers, humoral responses, tissue viral loads, and plasma viral antigens on days 1, 3, and 8. High-dimensional analyses, including RNA sequencing and flow cytometry, were performed on available samples. Mediation analyses were used to assess relationships between SAEs, baseline-adjusted biomarkers, and treatment-vaccination status.
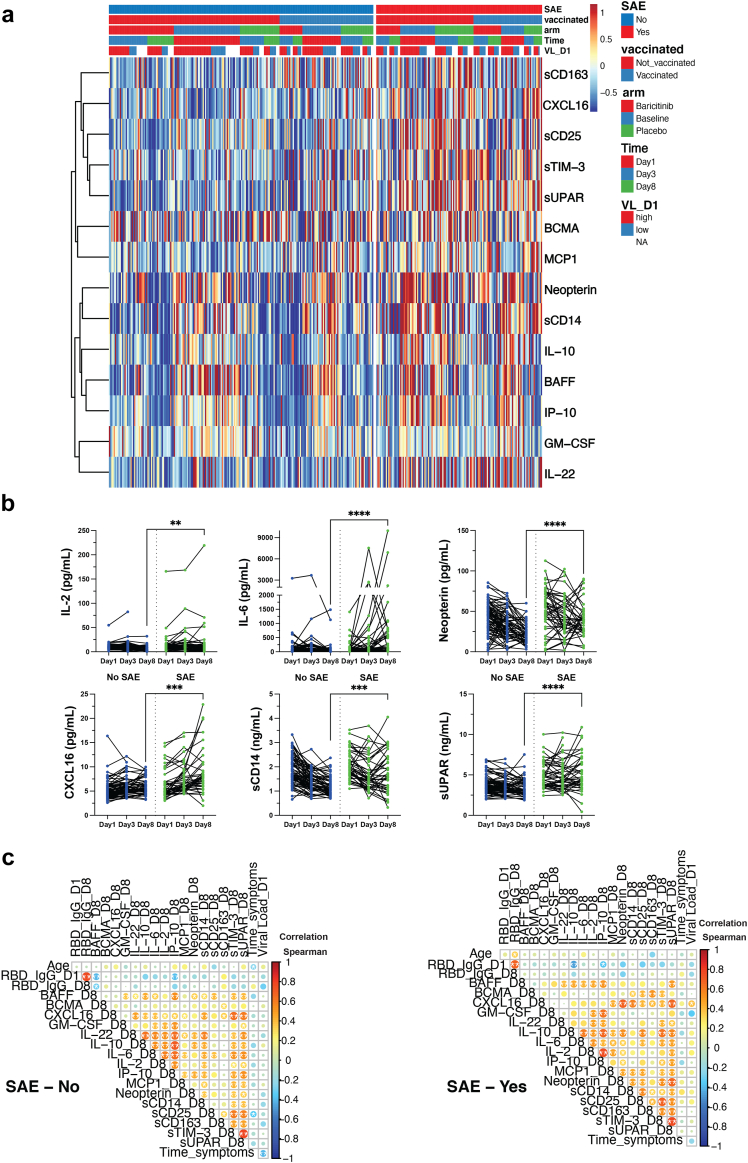
Findings: Vaccinated participants were older, more frequently hospitalized, had more comorbidities, and exhibited higher nasopharyngeal viral loads. Baricitinib treatment did not affect antibody responses or viral clearance, but reduced markers of T-cell and monocyte activation compared to placebo (sCD25, sCD14, sCD163, sTIM-3). Age, baseline levels of plasma viral antigen, and several inflammatory markers, as well as IL-2, IL-6, Neopterin, CXCL16, sCD14, and suPAR on day 8 were associated with the occurrence of SAEs. However, mediation analyses of markers linked to SAEs, baricitinib treatment, or vaccination status did not reveal statistically significant interactions between vaccination status and SAEs.
Interpretation: This sub-study did not identify any virus- or host-related biomarkers significantly associated with the interaction between SARS-CoV-2 vaccination status and the safety of baricitinib. However, caution should be exercised due to the moderate sample size.
Funding: EU Horizon 2020 (grant number 101015736).
Keywords: Baricitinib; COVID-19; Immunomodulation; Inflammation; JAK/STAT-inhibitor; SARS-CoV-2 vaccination; Serious adverse events.
Copyright © 2024. Published by Elsevier B.V.
Conflict of interest statement
Declaration of interests MT has been a pro bono member of the scientific advisory board for Lilly. JP reports lecture fees from Gilead, Shionogi, and Mundipharma, as well as payment for expert testimony from Gilead, Shionogi, Eumedica, and Pfizer, and support for attending meetings from Gilead, and Shionogi. ARH reports personal fee from Pfizer (2021) for lectures outside the submitted work. RP reports personal fees from MSD (2024) for one lecture and from Gilead (2023) and Pfizer (2023) for congress attendance. LAM reports Helse Sør-Øst UiO and Research Council of Norway grant for developing cellular analyses of COVID-19 (2020–2022), grant from KG Jebsen Stiftelsen, and grant from The Coalition for Epidemic Preparedness Innovation to monitor immune responses in patients (2021–2023). DC reports personal fees from Pfizer (2022) for a lecture outside the submitted work. BD reports support from Amgen for congress attendance. J-FT report honoraria from Shionogi, Merck, Pfizer, and Advanz as well as participation in advisory board for Gilead, Merck, Menarini, and Biomerieux. AEM reports stocks in Pfizer. LP reports honoraria from Gilead, GSK, Moderna, Pfizer, and ViiV Healthcare, as well as support for attending meetings from MSD and Pfizer. YZ reports payments for lectures from Gilead, Shionogi, and Mundipharma, payment for expert testimony from Gilead, Shionogi, Eumedica, and Pfizer, as well as support for attending meetings from Gilead and Shionogi. MB reports support for attending meetings from Gilead and Shionogi. JM reports support for attending meetings from Pfizer and Menarini as well as participation in advisory board for MSD. All other authors have nothing to declare.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
