

Development and validation of a prediction model for intrapartum fever related to chorioamnionitis in parturients undergoing epidural analgesia
- PMID: 39732828
- PMCID: PMC11682342
- DOI: 10.1038/s41598-024-82722-y
Development and validation of a prediction model for intrapartum fever related to chorioamnionitis in parturients undergoing epidural analgesia
Abstract
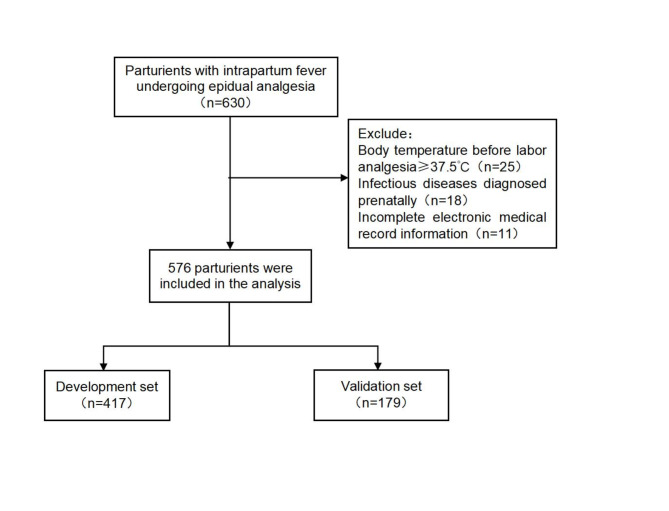
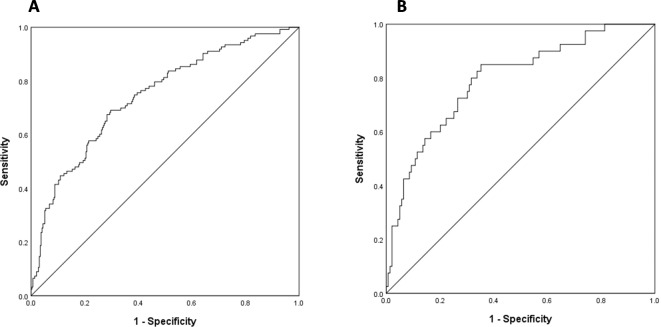
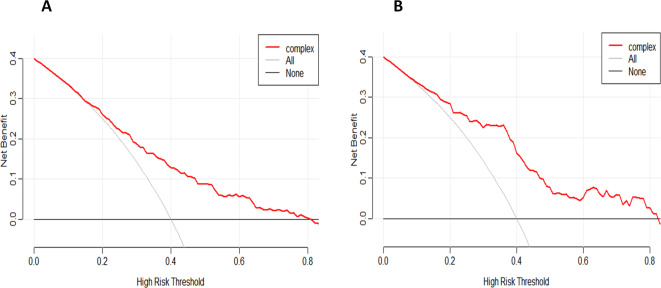
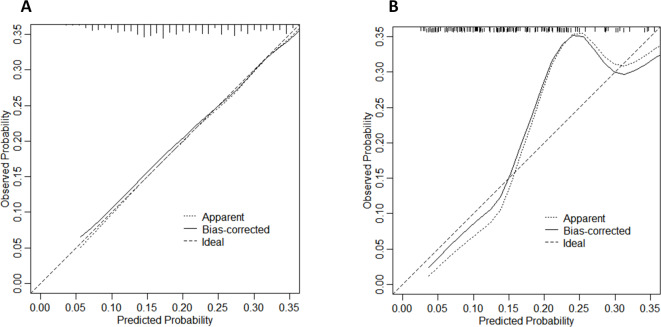
Intrapartum fever is a common complication in parturients undergoing epidural analgesia (EA), significantly increasing the incidence of maternal and infant complications. This study aims to develop and validate a prediction model for intrapartum fever related to chorioamnionitis (IFTC) in parturients undergoing epidural analgesia. A total of 596 parturients with fever (axillary temperature ≥ 38℃) who received EA from January 2020 to December 2023 were included and randomly assigned to the training set (N = 417) and the validation set (N = 179) according to the ratio of 7:3. The independent risk factors were screened by univariate and multivariate logistic regression analysis to develop a nomogram model. Decision curve analysis (DCA) was used to evaluate the clinical effectiveness and discrimination of the model; calibration curve was used to assess the accuracy of the model. Maximum temperature, meconium-stained amniotic fluid, C-reactive protein (CRP), gestational age and BMI were independent risk factors for predicting IFTC, and the area under receiver operating characteristic curve (AUC) of the training set and the validation set were 0.744 (0.691-0.796) and 0.793 (0.714-0.872), respectively. The calibration curve showed good consistency between predicted and actual results. DCA curve showed that the model had clinical value throughout a broad threshold probability range. The nomogram prediction model based on CRP, meconium-stained amniotic fluid, maximum temperature, gestational age and BMI has good predictive performance for the risk of IFTC in EA parturients.
Keywords: Analgesia; Chorioamnionitis; Epidural; Fever; Labor pain; Prediction.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
