

Effect of enhanced external counterpulsation versus individual shear rate therapy on the peripheral artery functions
- PMID: 39732867
- PMCID: PMC11682309
- DOI: 10.1038/s41598-024-82485-6
Effect of enhanced external counterpulsation versus individual shear rate therapy on the peripheral artery functions
Abstract
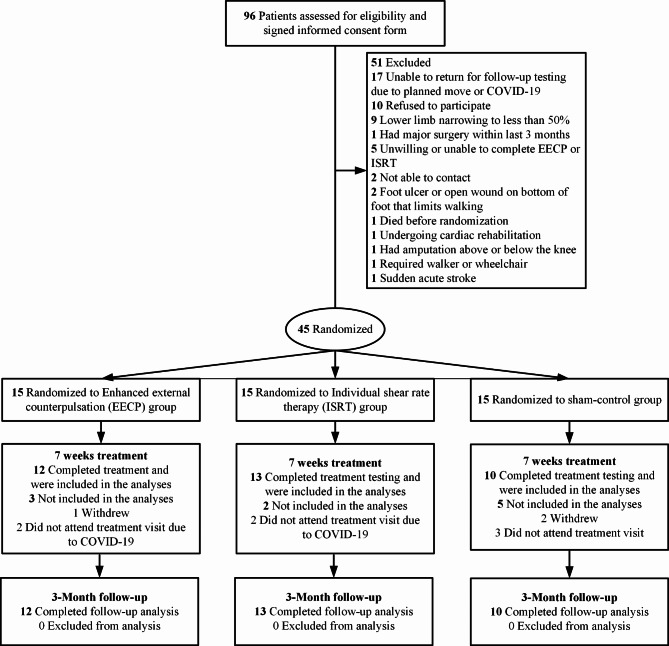
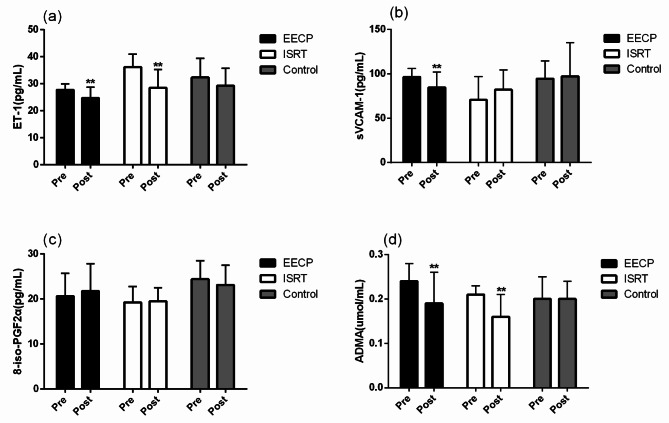
In this study, we aimed to assess the effects of enhanced external counterpulsation (EECP) and individual shear rate therapy (ISRT) on peripheral artery function in patients with lower extremity atherosclerotic disease (LEAD). We randomly assigned 45 LEAD patients to receive 35 sessions of 45 min of EECP (n = 15), ISRT (n = 15), or sham-control (n = 15). Flow-mediated dilation in the brachial artery (brachial-FMD); 6-min walk distance; blood flow in the popliteal, posterior tibial, anterior tibial, and dorsalis pedis arteries; and plasma levels were measured before and after the 7 weeks treatment. 36-item Short Form Health Survey [SF-36] was analyzed before, after 7 weeks, and 3-month follow-ups. EECP treatment significantly improved brachial-FMD and quality of life, increased walking distance, and increased blood flow and the diameters of the popliteal artery and posterior tibial artery (all P < 0.01). Conversely, ISRT markedly increased blood flow in the anterior tibial artery (P < 0.05). EECP and ISRT decreased the endothelin-1 and asymmetrical dimethylarginine levels in patients with LEAD (both P < 0.01). Additionally, sVCAM-1 was significantly reduced after EECP intervention (P = 0.004). Our findings demonstrate that EECP and ISRT have beneficial effects on walking distance, quality of life, flow-mediated dilation, endothelial-derived vasoactive agents, and inflammatory and oxidative stress in LEAD patients.Date of registration: 2021-06-21. Trial registration: ChiCTR2100048086.
Keywords: Enhanced external counterpulsation; Individual shear rate therapy; Lower extremity atherosclerotic disease; Vascular hemodynamics; Walking distance.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures



References
-
- Fihn, S. D. et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American college of cardiology foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and interventions, and Society of thoracic surgeons. J. Am. Coll. Cardiol.60 (24), e44–e164 (2012). - DOI - PubMed
-
- Cardiovascular disease prevention and control research center. Ministry of Health. China Cardiovascular Disease Report: China Cardiovascular Disease Report ([M], 2014).
Publication types
MeSH terms
Grants and funding
- Grant No. 82202292/National Natural Science Foundation of China
- No. A2022383/Guangdong Medical Science and Technology Research Foundation
- No.2021A1515110738/Guangdong Basic and Applied Basic Research Foundation
- ZDXKJF-01002/Shenzhen Key Clinical Discipline Funds
- No.2020YFC2004400/National Key Research and Development Program of China
LinkOut - more resources
Full Text Sources
