

Tuberculosis Preventive Treatment in High TB-Burden Settings: A State-of-the-Art Review
- PMID: 39733063
- PMCID: PMC11802714
- DOI: 10.1007/s40265-024-02131-3
Tuberculosis Preventive Treatment in High TB-Burden Settings: A State-of-the-Art Review
Abstract
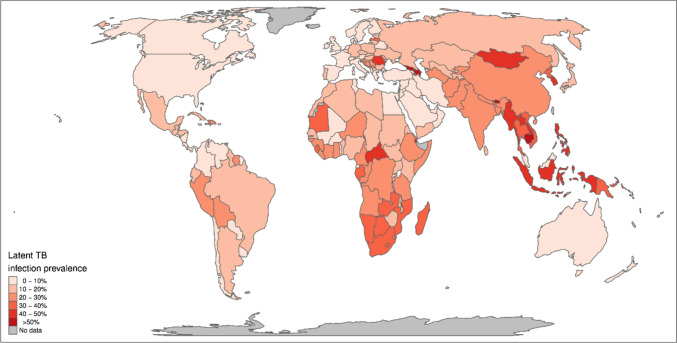
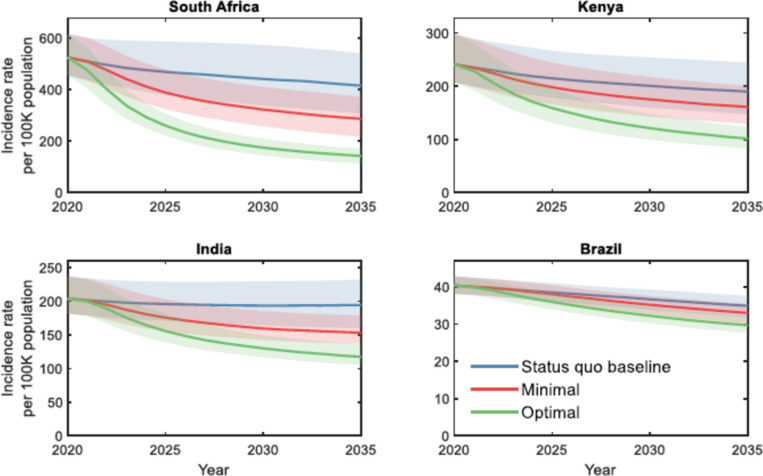
Tuberculosis (TB) is the leading cause of death from a single infectious agent. The burden is highest in some low- and middle-income countries. One-quarter of the world's population is estimated to have been infected with TB, which is the seedbed for progressing from TB infection to the deadly and contagious disease itself. Although some individuals may clear their infections through innate and acquired immunity, many do not. People living with HIV, TB-exposed household contacts, other individuals recently infected, and immunosuppressed individuals are at especially high risk of progressing to TB disease. There have been major advances in recent years to support the programmatic management of TB infection. New tests of infection, including those that predict progression to TB disease, have become available. Numerous World Health Organization-recommended TB preventive treatment (TPT) regimens are available for all ages and for both drug-susceptible and drug-resistant TB infection. All regimens are generally safe, efficacious, and cost effective and have a low risk of generating resistance. TPT is recommended for pregnant women who are at risk for developing TB, but some regimens are associated with an increased likelihood of poor obstetric and fetal outcomes, and newer regimens have not yet been tested in pregnancy. New formulations of rifapentine-based TPT have been developed, and the cost has been radically reduced. Innovative models of delivery to support the scale up of TPT have been developed. Modeling suggests that scaling up TPT, especially regimens with optimal target product profile characteristics, can contribute substantially to ending the TB epidemic. The global uptake of TPT has increased substantially, especially for people living with HIV. Implementation gaps remain, particularly for children, pregnant women, and other household contacts. Further innovation is required to support the continued scale up of TPT and to contribute to ending the TB epidemic.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Funding: GC and VC were supported by Unitaid through the IMPAACT4TB project (2017-20-IMPAACT4TB). GC is supported by an NIH grant UM1AI068636 for the PHOENIx MDR TB trial. REC was supported by Unitaid through the IMPAACT4TB project (2017-20-IMPAACT4TB) and NIH grant P30AI18436. KED is supported by NIH/NIAID K24AI150349. MG, AG, NSA, TR, CJH, SL, JSM, and VM have not received funding. Conflict of interest: VC, MG, AG, NSA, TR, CJM, JSM, VM, and KED have no relevant financial or non-financial interests to disclose. SML is funded by Merck through her institution for C19-related research and declares UpToDate—royalties for a chapter on TB infection in pregnancy. REC’s spouse owns stock in Merck. RC and GC have consulted for Johnson & Johnson. Availability of data and material: No data are available as this was a review. Ethics approval: Not applicable. The manuscript is a review and does not report results of a study that involved human participants, their data, or biological material. Consent for publication: Not applicable. The manuscript does not contain identifiable patient data. Consent for publication: Not applicable. The article does not contain clinical photos of patients or patient data that could be identifiable. Author contributions: VC and GC conceptualized and designed the outline of the paper. All authors (VC, MG, AG, NSA, TR, CJM, SL, JSM, VM, KED, REC, GC) contributed to specific sections of the manuscript and reviewed the paper. All authors read and approved the final version.
Figures

References
-
- World Health Organization. Global tuberculosis report 2024. Geneva: World Health Organization; 2024.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
