

Association between stress hyperglycemia ratio and mortality in patients with heart failure complicated by sepsis
- PMID: 39733142
- PMCID: PMC11682349
- DOI: 10.1038/s41598-024-82890-x
Association between stress hyperglycemia ratio and mortality in patients with heart failure complicated by sepsis
Abstract
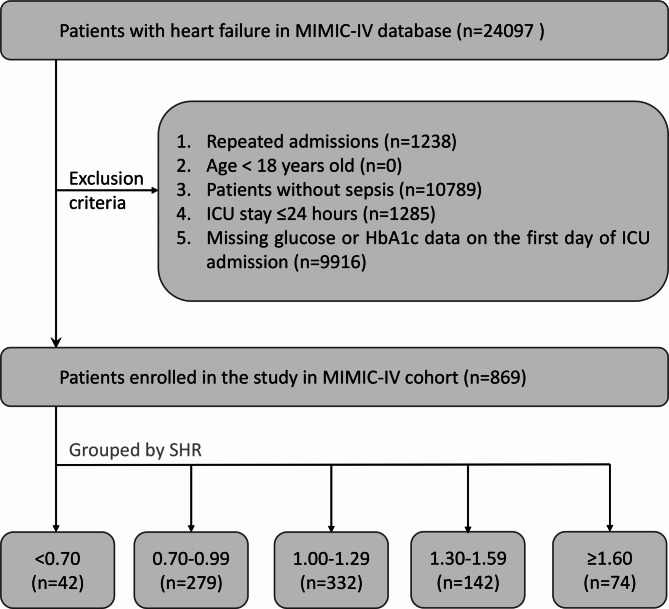
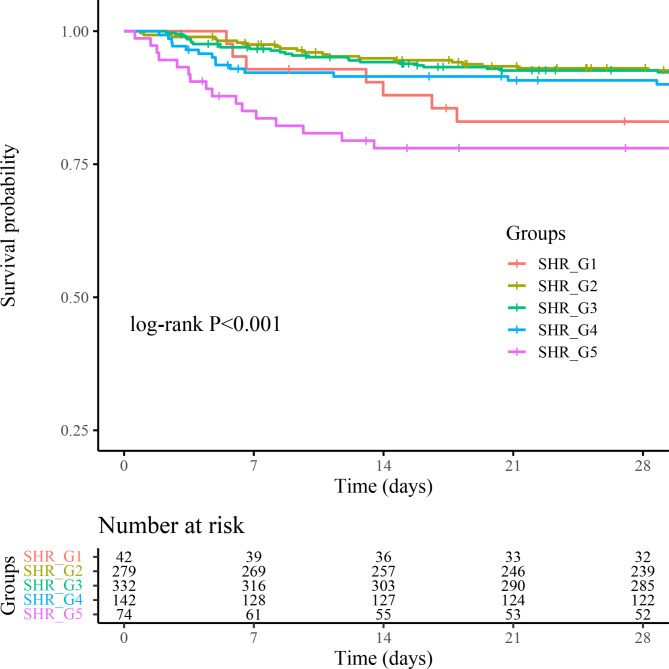
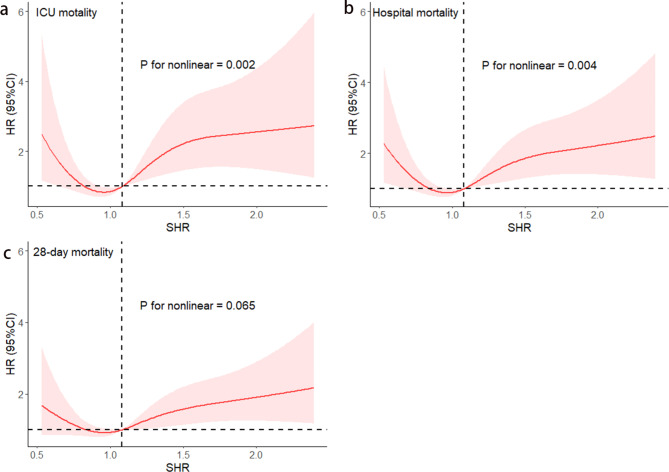
Individuals afflicted with heart failure complicated by sepsis often experience a surge in blood glucose levels, a phenomenon known as stress hyperglycemia. However, the correlation between this condition and overall mortality remains unclear. 869 individuals with heart failure complicated by sepsis were identified from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database and categorized into five cohorts based on their stress hyperglycemia ratio (SHR). The primary endpoints evaluated were mortality within the intensive care unit (ICU), all-cause mortality within 28 days, and all-cause mortality during hospitalization. Cox proportional hazards regression and restricted cubic spline analyses were employed to unravel the association between SHR and mortality. The ICU mortality, in-hospital mortality, and 28-day all-cause mortality were 10.01%, 13.69%, and 16.46%, respectively. Multivariable Cox proportional hazards regression analysis revealed a significant association between elevated SHR and all-cause mortality. After adjusting for confounding variables, elevated SHR was significantly associated with increased risk of ICU mortality (hazard ratio [HR] = 1.67; 95% confidence interval [CI], 1.03-2.70)), in-hospital mortality (HR = 1.53; 95% CI, 1.00-2.33)), and 28-day all-cause mortality (HR = 1.49; 95% CI, 1.02-2.17)). Restricted cubic spline analysis demonstrated a significant U-shaped relationship between SHR and the risk of all-cause mortality. This study revealed that stress hyperglycemia ratio is an independent prognostic factor in patients with heart failure complicated by sepsis. Notably, both very high and very low SHR values were associated with increased mortality risk.
Keywords: Heart failure; MIMIC-IV; Mortality; Sepsis; Stress hyperglycemia ratio.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The utilization of the MIMIC-IV database was sanctioned by the review boards of both the Massachusetts Institute of Technology and Beth Israel Deaconess Medical Centre. Given the public availability of the data within the MIMIC-IV database, the study was exempt from the need for an ethics approval statement and informed consent. Competing interests: The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
