

The natural history of portal venous system aneurysms
- PMID: 39733830
- PMCID: PMC12245757
- DOI: 10.1016/j.jvsv.2024.102163
The natural history of portal venous system aneurysms
Abstract
Background: Portal venous system aneurysms (PVAs) are increasingly diagnosed on cross-sectional computed tomography imaging. However, the natural history of these aneurysms is poorly understood, and reports are limited to small case series.
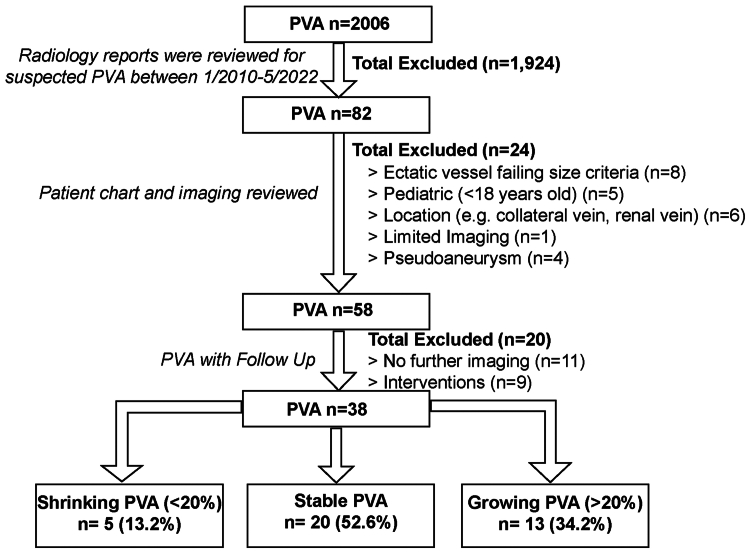
Methods: Terms relevant to PVAs were searched in radiology reports (2010-2022), with PVA presence confirmed by manual review. PVA were defined as a diameter greater than 1.5 cm in patients without cirrhosis and 1.9 cm in those with cirrhosis. Aneurysm growth was defined as greater than 20% increase in size, whereas aneurysm regression was defined as greater than 20% decrease in size. Patient demographics, comorbid conditions, and PVA outcomes were abstracted. Univariate statistics were used to compare groups.
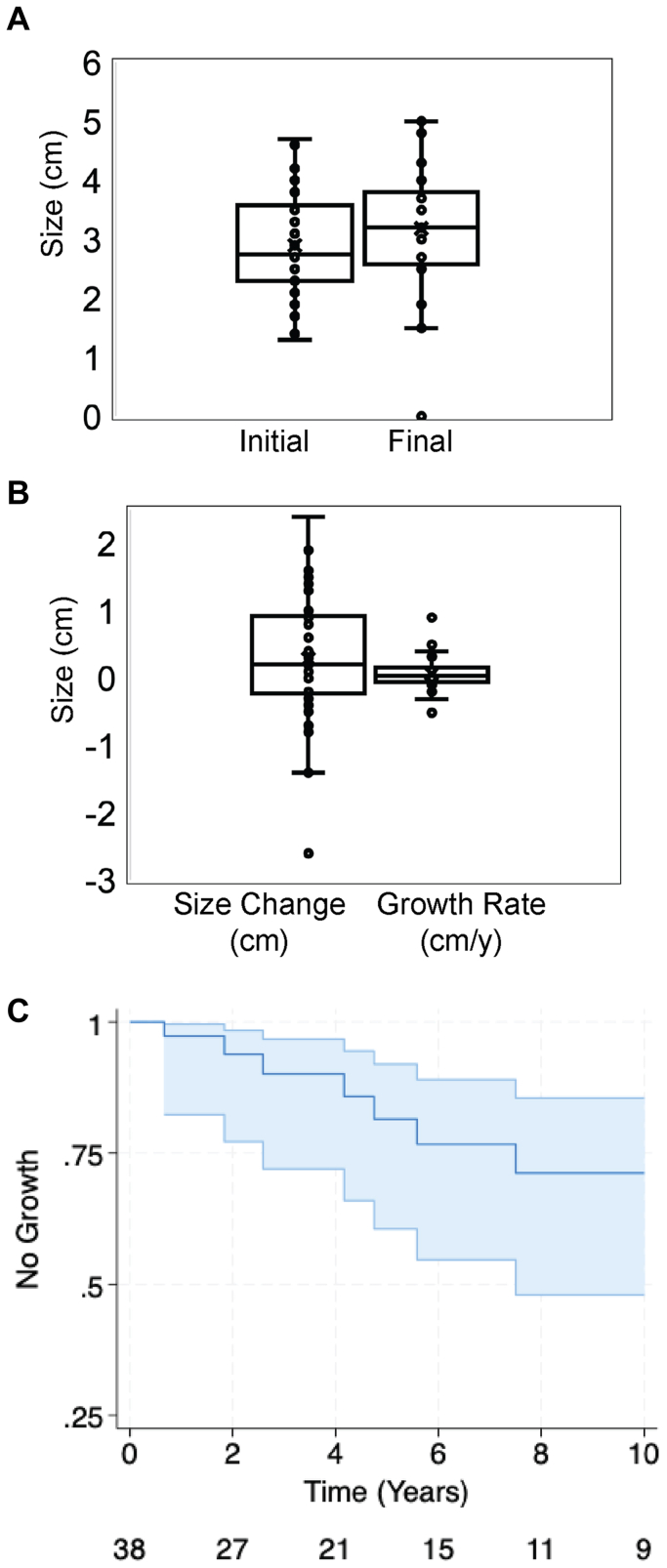
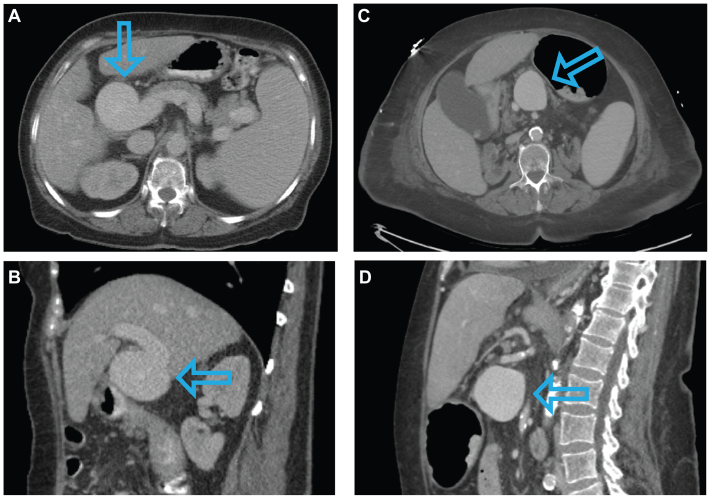
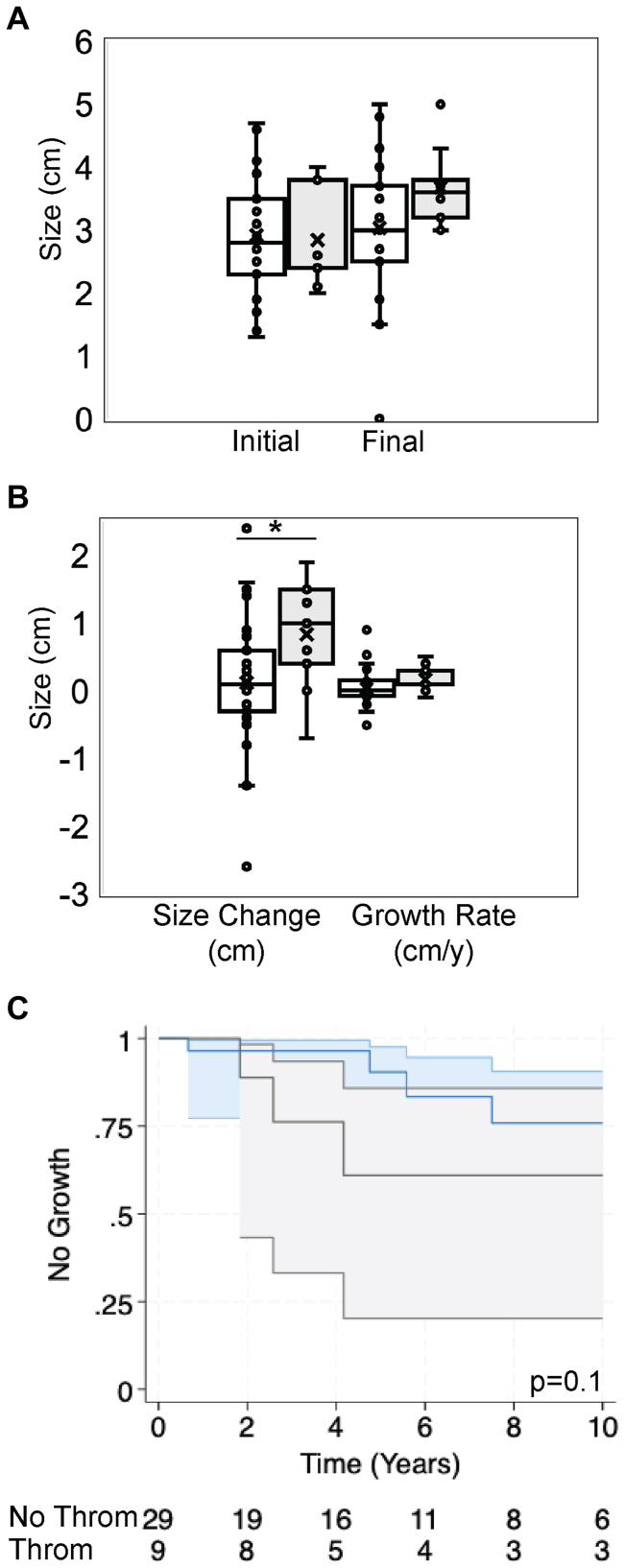
Results: Thirty-eight aneurysms with radiographic follow up were identified in 35 patients, involving the portal vein (n = 18; 47.4%), splenic vein (n = 10; 26.3%), superior mesenteric vein (n = 3; 7.9%), and portal confluence (n = 7; 18.4%). Although 12 (31.6%) were idiopathic, the remaining 26 (68.4%) were associated with portal hypertension (n = 20; 52.6%) and prior liver transplant (n = 4; 10.5%). The median growth was 0.2 cm (range, -2.6 to 2.4 cm) over median follow up over 5.0 years (range, 0.3-16.6 years). Five PVAs (13.2%) regressed and were largely idiopathic (80.0%; P = .03). Thirteen PVAs (34.2%) grew and were associated with portal hypertension (n = 11; 84.6%; P = .003) and thrombosis (n = 6; 46.2%; P = .05). Nine PVAs (23.7%) thrombosed, predominantly in males (n =7; 77.8%). The median growth was 1.0 cm (range, -0.7 to 1.9 cm). Three patients (33.3%) were symptomatic from PVA thrombosis including abdominal pain (n = 2; 22.2%), intestinal ischemia (n = 1; 11.1%), and variceal bleeding (n = 2; 22.2%). Four patients (44.4%) were treated with anticoagulation. No aneurysms ruptured. Of the 58 PVAs initially identified with and without radiographic follow up, five (8.6%) underwent intervention with a median diameter of 4.0 cm (range, 3.4-5 cm). Intervention included vein ligation (n = 1; 20.0%), aneurysmorrhaphy (n = 1; 20.0%), and aneurysmectomy (n = 3; 60.0%). There was one case of aneurysm recurrence 20 years following resection and one postoperative mortality.
Conclusions: Two-thirds of PVAs, including those with size greater than 3 cm, remain stable on surveillance. Although annual surveillance is initially recommended to confirm PVA stability, interval imaging can be subsequently extended given low growth rates. Over 20% of PVAs thrombosed, but none ruptured. Although we did not observe any cases of rupture, the devastating consequences of rupture necessitate consideration of surgical intervention for large symptomatic PVAs.
Keywords: Portal vein aneurysm; Portal venous system; Splanchnic vein thrombosis; Splenic vein aneurysm.
Copyright © 2025 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures None.
Figures

References
-
- Koc Z., Oguzkurt L., Ulusan S. Portal venous system aneurysms: imaging, clinical findings, and a possible new etiologic factor. AJR Am J Roentgenol. 2007;189:1023–1030. - PubMed
-
- Laurenzi A., Ettorre G.M., Lionetti R., Meniconi R.L., Colasanti M., Vennarecci G. Portal vein aneurysm: what to know. Dig Liver Dis. 2015;47:918–923. - PubMed
-
- Sfyroeras G.S., Antoniou G.A., Drakou A.A., Karathanos C., Giannoukas A.D. Visceral venous aneurysms: clinical presentation, natural history and their management: a systematic review. Eur J Vasc Endovasc Surg. 2009;38:498–505. - PubMed
-
- Ahmed O., Ohman J.W., Vachharajani N., et al. Feasibility and safety of non-operative management of portal vein aneurysms: a thirty-five year experience. HPB (Oxford) 2021;23:127–133. - PubMed
-
- Chau P., Yoon J.S., Moses D., Pather N. A systematic review and meta-analysis of portal vein morphometry in pediatric and adult populations: drawing the line between normal and abnormal findings. Eur J Radiol. 2023;168 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
