

Development and verification of a nomogram for recurrence risk of Benign Paroxysmal Positional Vertigo in middle-aged and older populations
- PMID: 39734629
- PMCID: PMC11671359
- DOI: 10.3389/fneur.2024.1483233
Development and verification of a nomogram for recurrence risk of Benign Paroxysmal Positional Vertigo in middle-aged and older populations
Abstract
Background: Benign Paroxysmal Positional Vertigo (BPPV) is the most common cause of peripheral vertigo, with frequent recurrence, particularly pronounced among middle-aged and elderly populations, significantly affecting patients' quality of life. This study aimed to identify predictive factors for recurrence in middle-aged and older patients with BPPV and to develop a nomogram prediction model based on these predictors.
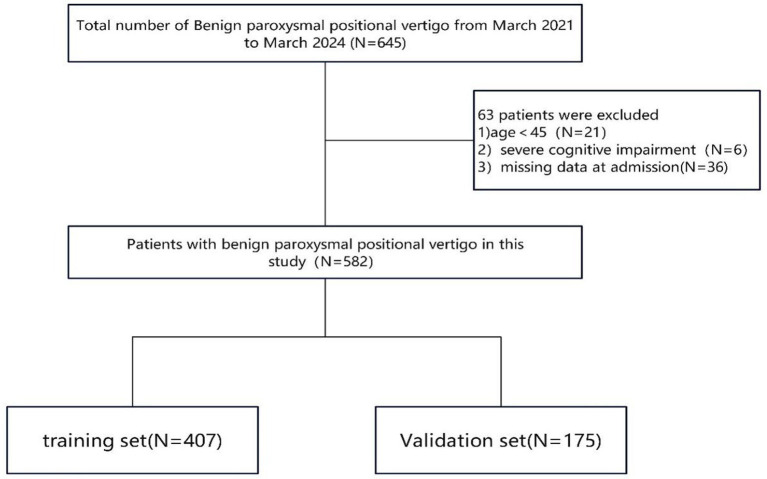
Methods: This retrospective study included 582 participants aged ≥45 years who were selected from the electronic medical records system of the First Hospital of Changsha between March 2021 and March 2024. Randomly chosen participants (n = 407, 70%) constituted the training group, whereas the remaining participants (n = 175, 30%) formed the validation group. This study used LASSO binomial regression to select the most predictive variables. A predictor-based nomogram was developed to calculate the risk of BPPV recurrence. The performance of the nomogram was evaluated using the area under the receiver operating characteristic curve (AUC) and calibration curves with 1,000 bootstrap resampling validations. Decision curve analysis (DCA) was conducted to assess the clinical usefulness of the nomogram.
Results: According to findings from least absolute shrinkage and selection operator (LASSO) binomial regression and logistic regression screening, older age, higher levels of uric acid (UA) and homocysteine (HCY), diabetes, migraine, anxiety, and insomnia were identified as independent factors associated with an increased recurrence risk of BPPV. A nomogram model for predicting recurrence risk was developed based on these predictors. The nomogram achieved an AUC (C-statistic) of 0.8974 (95% CI: 0.8603-0.9345) in the training group and 0.8829 (95% CI: 0.8253-0.9406) in the validation group. Calibration curves, after 1,000 bootstrap resamples, demonstrated good agreement between the predicted and actual probabilities in the development and validation cohorts. DCA indicated that the nomogram had clinical utility.
Conclusion: The nomogram model incorporating age, UA, HCY, diabetes, migraine, anxiety status, and insomnia demonstrated a strong predictive capability for estimating the probability of BPPV recurrence in middle-aged and elderly patients. This tool is valuable for identifying individuals at high risk of BPPV recurrence and can aid physicians in making informed treatment decisions aimed at reducing recurrence rates.
Keywords: BPPV; Benign Paroxysmal Positional Vertigo; nomogram; recurrence; risk factors.
Copyright © 2024 Tang, Zhang, Wang, Luo, He, Xiong and Yu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
-
- Fife TD, Iverson DJ, Lempert T, Furman JM, Baloh RW, Tusa RJ, et al. Practice parameter: therapies for benign paroxysmal positional vertigo (an evidence-based review): report of the quality standards subcommittee of the american academy of neurology. Neurology. (2008) 70:2067–74. doi: 10.1212/01.wnl.0000313378.77444.ac, PMID: - DOI - PubMed
-
- De Stefano A, Dispenza F, Suarez H, Perez-Fernandez N, Manrique-Huarte R, Ban JH, et al. A multicenter observational study on the role of comorbidities in the recurrent episodes of benign paroxysmal positional vertigo. Auris Nasus Larynx. (2014) 41:31–6. doi: 10.1016/j.anl.2013.07.007, PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources