

First Documented Successful Treatment of Chronic Postoperative Fungal Endophthalmitis Induced by Trichosporon Inkin with Fluconazole
- PMID: 39734738
- PMCID: PMC11681906
- DOI: 10.2147/IDR.S485152
First Documented Successful Treatment of Chronic Postoperative Fungal Endophthalmitis Induced by Trichosporon Inkin with Fluconazole
Abstract
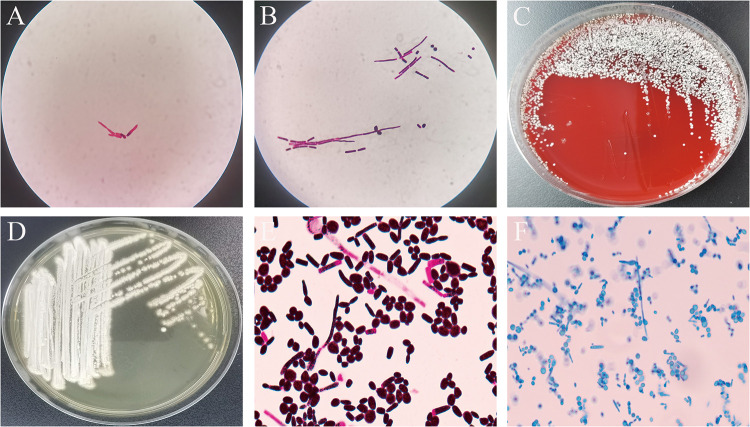
This report details an uncommon occurrence of chronic endophthalmitis following cataract surgery attributed to an infection by Trichosporon inkin (T. inkin). The infection was identified through MALDI-TOF mass spectrometry along with sequencing analysis. Although the patient exhibited a robust immune response, the infection escalated quickly from the right eye to the left. Treatment involved vitrectomy and peeling surgery on the right eye, paired with systemic fluconazole antifungal therapy and intravitreal injection, resulting in significant recovery. The visual acuity of the right eye enhanced from finger counting to 20/63. This account represents the inaugural documented instance of endophthalmitis caused by T. inkin that was effectively managed with fluconazole. This underscores the critical role of vitreous humor enrichment culture and antifungal susceptibility testing of T. inkin in the treatment of endophthalmitis.
Keywords: MALDI-TOF; Trichosporon inkin; endophthalmitis; fluconazole; matrix-assisted laser desorption ionization time of flight.
© 2024 Fan et al.
Conflict of interest statement
The authors state that the study was carried out without any commercial or financial ties that might be interpreted as a possible conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
