

Expression of Monocytes Subsets in Patients Diagnosed With Coronary Artery Atherosclerosis and Their Impact on Disease Severity
- PMID: 39734983
- PMCID: PMC11681966
- DOI: 10.7759/cureus.74670
Expression of Monocytes Subsets in Patients Diagnosed With Coronary Artery Atherosclerosis and Their Impact on Disease Severity
Abstract
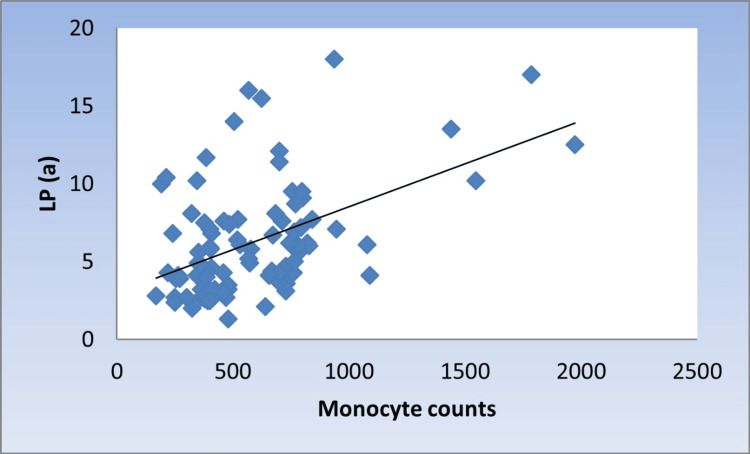
Introduction Many studies have supported inflammation as a mediator of lipoprotein (a) (Lp(a)) induced increase in cardiovascular disease risk, as it has pro-inflammatory effects on endothelial cells and monocytes. Aim This study aims to correlate Lp(a) level with different monocyte subsets in coronary atherosclerotic patients with different severity. Method The study included 60 patients with a mean age of 53.1 ± 10.5 diagnosed as coronary atherosclerotic patients by coronary angiography. Lp levels were measured using enzyme-linked immunosorbent assay (ELISA), while blood counts and monocyte subsets were analyzed by flow cytometry, and 30 apparently healthy individuals were included as the control group. Results Patients showed significantly higher median monocytic %, Lp(a), and higher C-reactive protein (CRP) values than the control group. Patients were subdivided into two groups: normal Lp(a) < 6.2 mg/dL (n = 24) and hyperlipoproteinemia(a) (hyper Lp(a)) ≥ 6.2 mg/dL (n = 36). Patients with hyper Lp(a) had higher non-classical monocytes (31.5% vs. 20%). Coronary atherosclerosis severity was associated with higher Lp(a) levels as well as non-classical monocytes; patients with mild atherosclerosis showed the highest classical and intermediate subset levels. While for a non-classical subset, patients with severe atherosclerosis showed the highest median level. A significant moderate positive correlation between Lp(a) and monocyte counts, as well as monocyte-lymphocyte (M/L) index and non-classical monocytes, was found. Conclusions Hyper Lp(a) and increased count of non-classical monocytes are significantly increased with disease progression (triple-vessel coronary disease risk). These results suggest that the expansion of non-classical monocytes is a cardiovascular disease (CVD) risk and predictor for disease severity. Strategies targeting inflammatory monocytes may slow CVD progression.
Keywords: atherosclerosis; cd16+ monocytes; flow cytometery; lipoprotein (a); non classical monocytes.
Copyright © 2024, Kamel et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Minia University, Faculty of Medicine, Institutional Review Board "MUFMIRB" issued approval 133:11/2021. You are kindly informed that this letter has been issued to officially notify you that our Minia University, Faculty of Medicine, Institutional Review Board "MUFMIRB," has reviewed and approved your submitted research documents. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures




References
-
- Periodic and intermittent fasting in diabetes and cardiovascular disease. Crupi AN, Haase J, Brandhorst S, Longo VD. Curr Diab Rep. 2020;20:83. - PubMed
-
- Lipoprotein(a) and inflammation - pathophysiological links and clinical implications for cardiovascular disease. Simantiris S, Antonopoulos AS, Papastamos C, Benetos G, Koumallos N, Tsioufis K, Tousoulis D. J Clin Lipidol. 2023;17:55–63. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous