

Left Atrial Appendage Closure With Catheter Ablation vs. Ablation Alone on Outcomes of Atrial Fibrillation in Heart Failure With Reduced Ejection Fraction: A Propensity Score-Matched Analysis
- PMID: 39735150
- PMCID: PMC11673331
- DOI: 10.7759/cureus.74577
Left Atrial Appendage Closure With Catheter Ablation vs. Ablation Alone on Outcomes of Atrial Fibrillation in Heart Failure With Reduced Ejection Fraction: A Propensity Score-Matched Analysis
Abstract
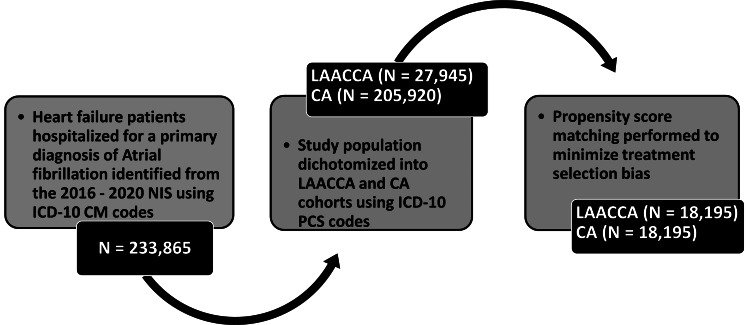
Background Combining left atrial appendage closure with catheter ablation (LAACCA) has been proposed as a potential approach to improving outcomes by simultaneously addressing arrhythmia and reducing stroke risk. This study compares the in-hospital outcomes of LAACCA vs. catheter ablation (CA) alone for atrial fibrillation (AFib) in patients with heart failure with reduced ejection fraction (HFrEF). Methods We analyzed adult hospitalizations with HFrEF and AFib who underwent LAACCA or CA alone from the 2016-2020 nationwide inpatient sample using validated ICD-10 codes. Propensity score matching, accounting for patient-, hospital-, and procedure-level covariates, illness severity, and baseline risk of mortality, was used to alleviate bias in nonrandomized treatment assignments. The primary endpoints included all-cause in-hospital mortality, hospital stay, and hospitalization costs. Secondary endpoints included postprocedural complication rates. Prolonged hospitalization was defined as hospital stay in the top decile of hospital stay in each cohort. All statistical analyses in the study were based on weighted hospital data. Results About 233,865 HFrEF patients were hospitalized for AFib. Approximately 27,945 (11.9%) underwent LAACCA, while 205,920 (88.1%) underwent CA only. The cohort comprised mostly males (151,077; 64.6%) (mean age: 67.4; SD: 4.3). The propensity score-matched cohort comprised 18,195 LAACCAs and 18,195 CAs; all covariate imbalances were alleviated. LAACCA was associated with a higher rate of prolonged hospital stay (7.6 vs 5.6 days; P<0.001), a higher mortality rate (209 (1.1%) vs. 160 (0.9%); P=0.011), and higher mean hospital costs ($289,960 vs. $183,932; P<0.001) compared with CA alone. LAACCA was associated with a higher incidence of acute myocardial ischemia (528 (2.9%) vs. 455 (2.5%); P=0.013), complete atrioventricular block (1,200 (6.6%) vs. 892 (4.9%); P=0.004), need for implantable device therapy (1,510 (8.3%) vs. 1,348 (7.4%); P=0.017), pneumothorax (328 (1.8%) vs. 91 (0.5%); P<0.0001), hemothorax (200 (1.1%) vs. 127 (0.7%); P<0.0001), pneumonia (983 (5.4%) vs. 546 (3.0%); P<0.0001), vascular access complications (346 (1.9%) vs. 255 (1.4%); P=0.046), and septicemia (309 (1.7%) vs. 182 (1.0%); P<0.001). CA was associated with a greater incidence of cardiac tamponade (237 (1.3%) vs. 382 (2.1%); P=0.010) and femoral artery pseudoaneurysm (364 (0.2%) vs. 91 (0.5%); P<0.001). Conclusion LAACCA was correlated with higher mortality odds compared to CA alone for atrial fibrillation in HFrEF.
Keywords: atrial fibrillation; catheter ablation; electrocardiogram (ekg) atrial fibrillation (a-fib) with rapid ventricular response (rvr); heart failure; left atrial appendage closure.
Copyright © 2024, Uwumiro et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
LinkOut - more resources
Full Text Sources