

Prediction of Acute Kidney Injury After Cardiac Surgery With Combined Arterial and Venous Intrarenal Doppler
- PMID: 39735690
- PMCID: PMC11672484
- DOI: 10.1177/20543581241309976
Prediction of Acute Kidney Injury After Cardiac Surgery With Combined Arterial and Venous Intrarenal Doppler
Abstract
Background: Acute kidney injury (AKI) occurs in up to 50% of cardiac surgical patients and is often hemodynamically mediated. Point-of-care ultrasound is a non-invasive tool that has the potential to characterize intrarenal hemodynamics and predict the risk of AKI.
Objectives: We aimed to determine the predictive characteristics of intrarenal arterial and venous Doppler markers for postoperative AKI in cardiac surgical patients.
Design: This study is the secondary analysis of a prospective cohort study.
Setting: This study is carried out in a care academic cardiac surgical center in Montreal, Quebec, Canada.
Patients: Adult patients undergoing cardiac surgery with the use of cardiopulmonary bypass.
Measurements: Point-of-care ultrasound assessments were performed preoperatively and at intensive care unit admission. Arterial measurements included the renal resistive index (RRI) and intrarenal artery velocity-time integral normalized to peak systolic velocity (VTI/PSV). Venous measurements included intrarenal venous flow (IRVF) pattern and renal venous stasis index (RVSI).
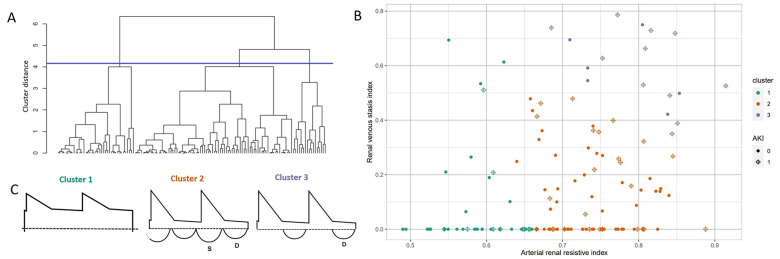
Methods: We used area under the receiving operating characteristic curves (AUCs) with net reclassification index (NRI) and multivariable logistic regression to determine predictive characteristics for postoperative AKI. Furthermore, we used hierarchical clustering to identify potential groups with similar Doppler parameters and performed comparisons of patients' characteristics and outcomes between groups.
Results: We included 136 patients with 47 (34.6%) developing postoperative AKI. At intensive care unit admission, arterial indices showed similar discrimination for the prediction of AKI (RRI: AUC = 0.64; 95% confidence interval (CI) = 0.55 to 0.74; and VTI/PSV: AUC = 0.67; 95% CI = 0.57 to 0.77). Venous Doppler indices including IRVF patterns (AUC = 0.64; 95% CI = 0.53 to 0.74) and RVSI (AUC = 0.60; 95% CI = 0.50 to 0.71) also showed similar performance. The combined model of RRI and IRVF pattern (AUC = 0.69; 95% CI = 0.59 to 0.78) improved the prediction of AKI compared to either RRI (NRI = 0.50; 95% CI = 0.17 to 0.84) or IRVF pattern (NRI = 0.38; 95% CI = 0.04 to 0.70) alone. Through hierarchical clustering, we identified 3 groups (1: low RRI, 2: high RRI/low RVSI, and 3: high RRI/high RVSI) with different patient characteristics and outcomes. The patient in group 3 had a higher risk of AKI and worse clinical outcomes compared with other groups.
Limitations: Single-center design in cardiac surgical patients limits generalizability.
Conclusions: Although more complex indices of intrarenal Doppler indices including the VTI/PSV and RVSI did not improve prediction of postoperative AKI, combining RRI and IRVF pattern improved risk prediction for AKI. Intrarenal arteriovenous Doppler subphenotypes identified patient groups at high risk of postoperative AKI.
Contexte: L’insuffisance rénale aiguë (IRA) survient chez jusqu’à 50 % des patients qui subissent une chirurgie cardiaque et elle est souvent médiée par hémodynamique. L’échographie au point d’intervention est un outil non effractif qui a le potentiel de caractériser l’hémodynamique intrarénale et de prédire le risque d’IRA.
Objectif: Notre objectif était de déterminer les caractéristiques prédictives des marqueurs Doppler artériels et veineux intrarénaux pour l’IRA postopératoire chez les patients en chirurgie cardiaque.
Type d’étude: Analyse secondaire d’une étude de cohorte prospective.
Cadre: Centre universitaire de soins tertiaires et de chirurgie cardiaque à Montréal (Québec, Canada).
Sujets: Patients adultes opérés sous pontage cardio-pulmonaire.
Mesures: Des échographies au point d’intervention ont été effectuées avant l’opération et à l’admission aux soins intensifs. Les mesures artérielles incluaient l’indice de résistance rénale (IRR) et l’intégrale vitesse-temps de l’artère intrarénale normalisée à la vitesse systolique maximale (IVT/VSM). Les mesures veineuses incluaient le profil veineux intrarénal (PVIR) et l’indice de stase veineuse rénale (ISVR).
Méthodologie: Nous avons utilisé la surface sous la courbe ROC (SSC) avec indice de reclassement net (NRI) et la régression logistique multivariée pour déterminer les caractéristiques prédictives de l’IRA postopératoire. Nous avons également utilisé le regroupement hiérarchique pour identifier des groupes montrant des paramètres Doppler similaires, puis nous avons procédé à la comparaison des caractéristiques des patients et des résultats entre les groupes.
Résultats: Nous avons inclus 136 patients dont 47 (34 %) ont développé une IRA postopératoire. À l’admission aux soins intensifs, les indices artériels (IRR et IVT/VSM) ont montré une discrimination similaire pour prédire l’IRA (SSC: 0,64 et 0,67 respectivement, avec intervalles de confiance à 95 % (IC95) de 0,55 à 0,74 et de 0,57 à 0,77). Les indices Doppler veineux, soit le PVIR (SSC: 0,64; IC95: 0,53 à 0,74) et l’ISVR (SSC: 0,60; IC95: 0,50 à 0,71), ont également montré des performances similaires. Le modèle combiné IRR + PVIR (SSC: 0,69; IC95: 0,59 à 0,78) a amélioré la prédiction de l’IRA par rapport à l’IRR seul (NRI: 0,50; IC 95: 0,17 à 0,84) ou au PVIR seul (NRI: 0,38; IC 95: 0,04 à 0,70). Avec le regroupement hiérarchique, nous avons identifié trois groupes (groupe 1: IRR faible; groupe 2: IRR élevé/ISVR faible; et groupe 3: IRR élevé/ISVR élevé) montrant des caractéristiques et des résultats différents pour les patients. Les patients du groupe 3 présentaient un risque plus élevé d’IRA et des résultats cliniques moins bons que ceux des autres groupes.
Limites: Le fait qu’il s’agit d’une étude monocentrique chez des patients en chirurgie cardiaque limite la généralisabilité.
Conclusion: Les indices plus complexes du Doppler intrarénal, notamment l’IVT/VSM et l’ISVR, n’ont pas amélioré la prédiction de l’IRA postopératoire, contrairement au modèle combiné IRR + PVIR. Les sous-phénotypes des Doppler artérioveineux intrarénaux ont permis d’identifier des groupes de patients qui présentent un risque élevé d’IRA postopératoire.
Keywords: acute kidney injury; cardiac surgery; point-of-care ultrasound.
© The Author(s) 2024.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf. WB-S reports receiving research funding from Displaid and consulting honoraria from GSK and Bayer. AD reports receiving a research grant from Edwards and consulting fees from CAE Healthcare and speaker honoraria from Masimo. The remaining authors declare no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years; and no other relationships or activities that could appear to have influenced the submitted work.
Figures


References
LinkOut - more resources
Full Text Sources
