

B-Acute Lymphoblastic Leukemia/Lymphoblastic Lymphoma Mimicking Fibrosing Mediastinitis: A Case Report and Diagnostic Insight
- PMID: 39736074
- PMCID: PMC11694771
- DOI: 10.12659/AJCR.945804
B-Acute Lymphoblastic Leukemia/Lymphoblastic Lymphoma Mimicking Fibrosing Mediastinitis: A Case Report and Diagnostic Insight
Abstract
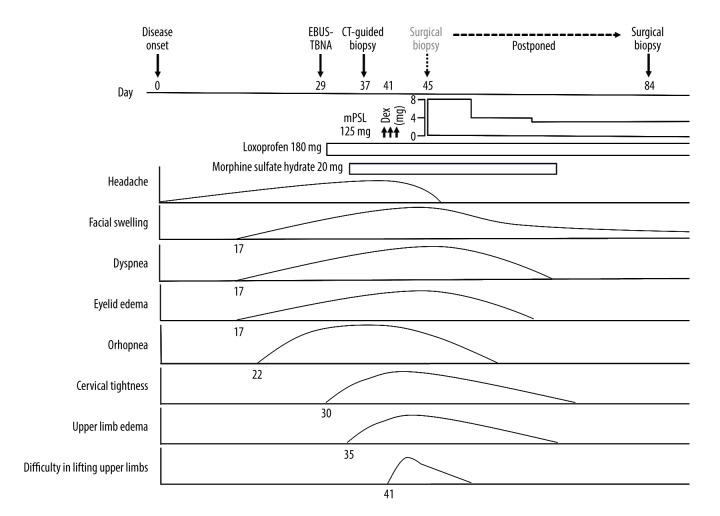
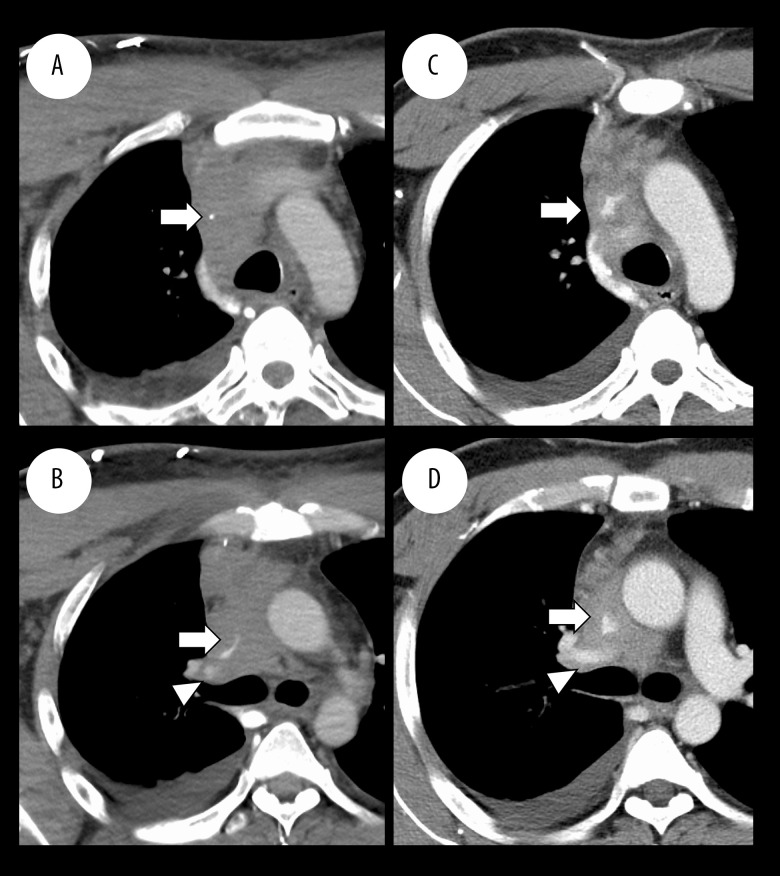
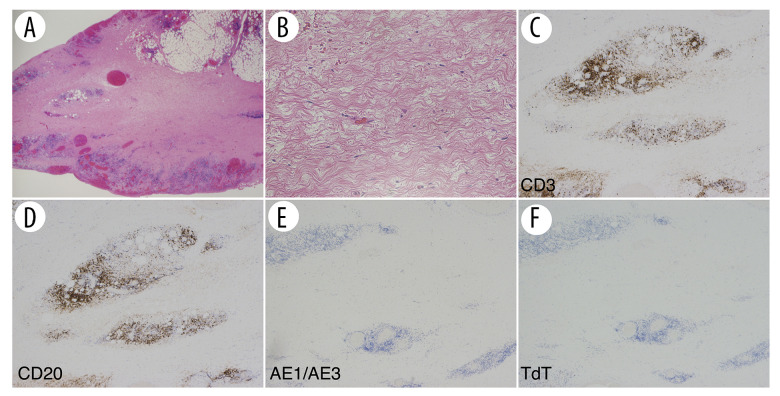
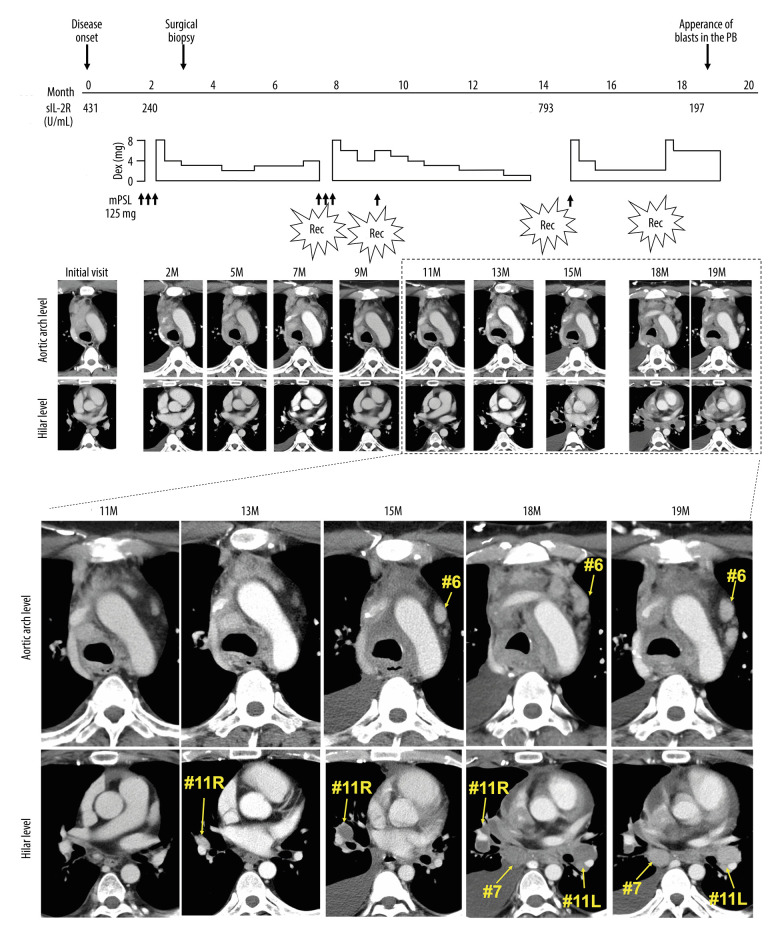
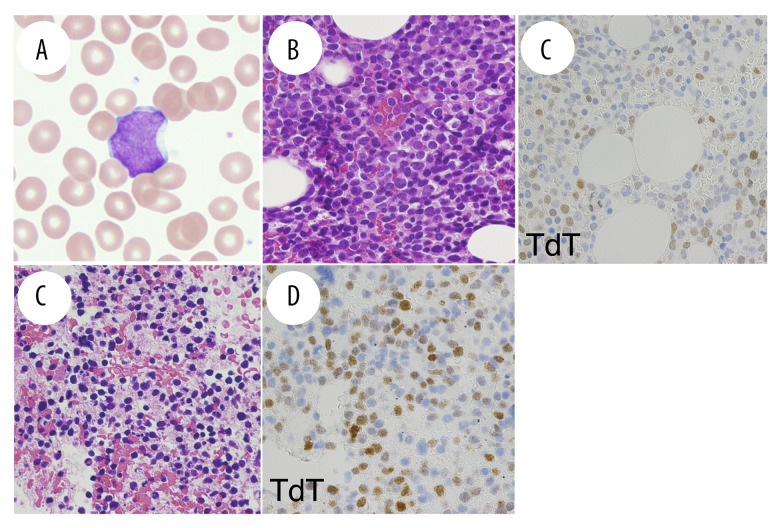
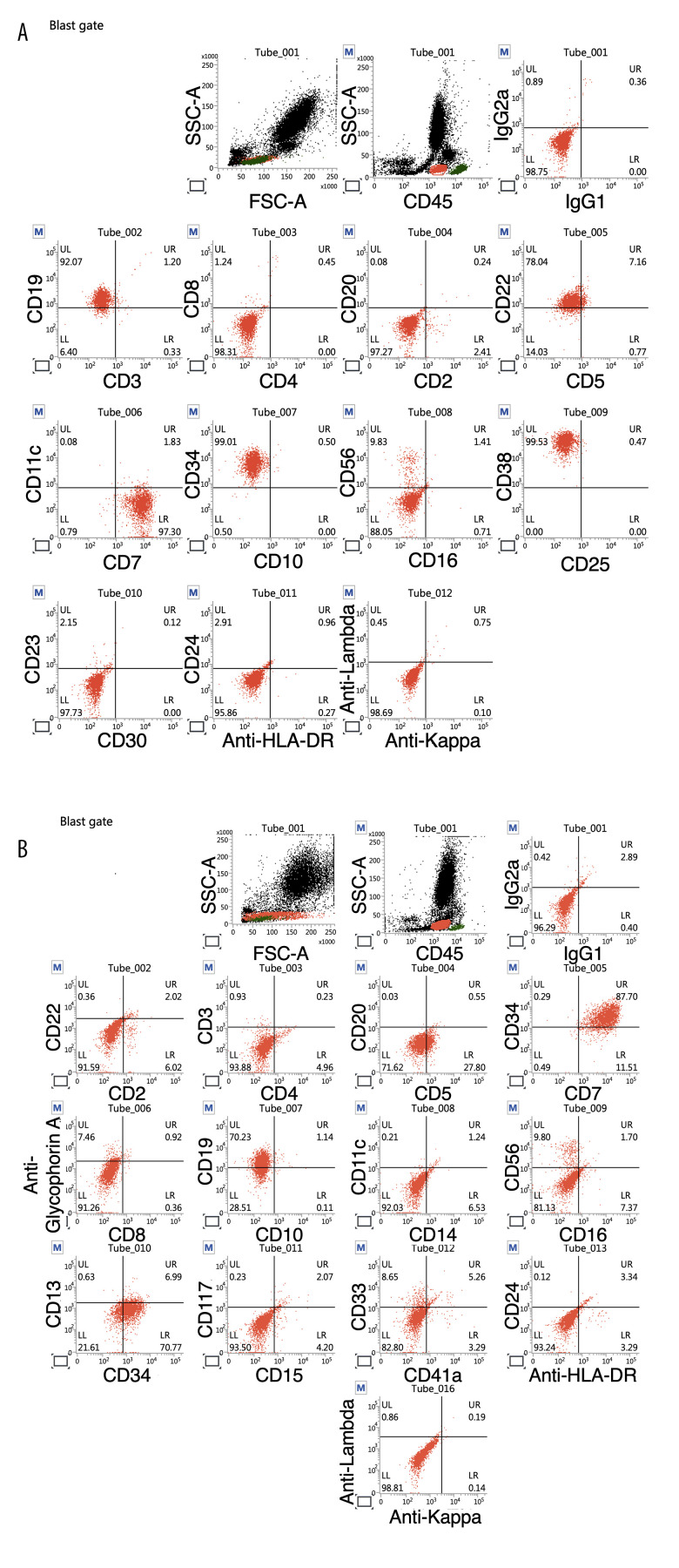
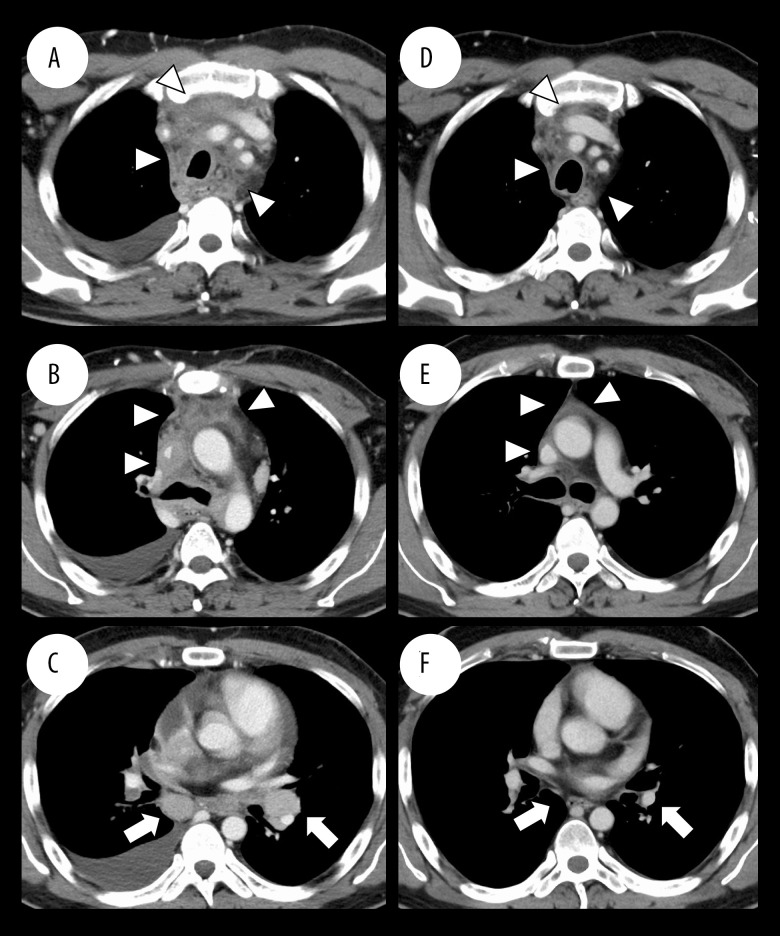
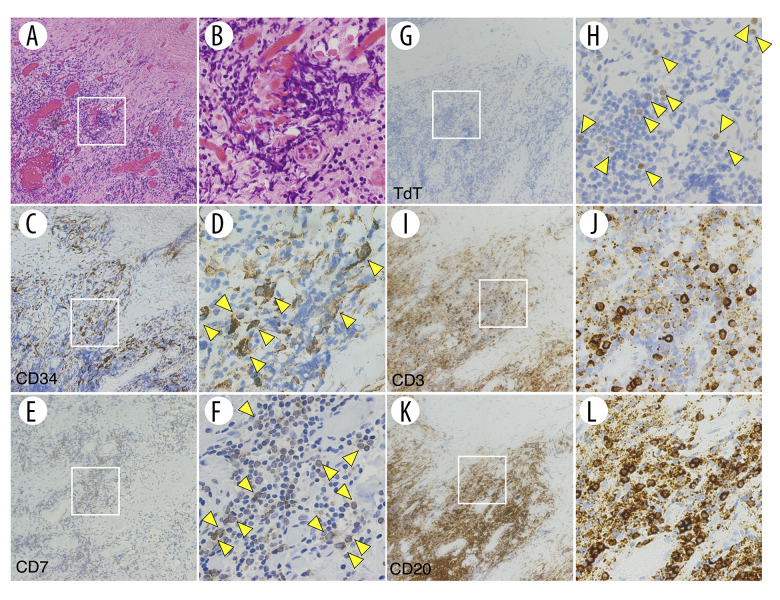
BACKGROUND Fibrosing mediastinitis (FM) is a rare, fibroproliferative disorder within the mediastinum. It is extremely rare for hematologic malignancies to develop as FM. CASE REPORT A 32-year-old Japanese man with a 1-month history of headache and 2-week history of facial swelling underwent chest computed tomography (CT); a diffuse mass-like lesion was revealed in the anterior mediastinum with severe stenosis of vital mediastinal organs. After a surgical biopsy, an initial diagnosis of idiopathic FM was made. The FM lesions responded mildly to corticosteroids but recurred repeatedly. Sixteen months after the treatment initiation, blasts appeared in the peripheral blood (PB), and the patient was diagnosed with B-acute lymphoblastic leukemia/lymphoblastic lymphoma (B-ALL/LBL). Chemotherapy led to complete remission of the B-ALL/LBL and almost complete disappearance of FM-like lesions. Immunohistochemistry of the mediastinal biopsy specimen taken before the blasts' appearance in PB demonstrated a CD34/CD7/terminal deoxynucleotidyl transferase-positive population, an identical pattern of expression common to the blasts in the patient's PB and bone marrow. CONCLUSIONS This is the first case report of B-ALL/LBL presenting as FM. This case underscores the importance of considering the possibility of latent hematologic malignancy even in the absence of new symptoms other than those caused by FM lesions for a long period of time. This is the first demonstration that leukemia cells may be present in the FM lesions from the initial stage of disease onset. Even if a diagnosis of idiopathic FM is confirmed, continued suspicion of the presence of hematologic malignancy is vital for improving patient outcomes.
Conflict of interest statement
Figures
References
-
- Goodwin RA, Nickell JA, Des Prez RM. Mediastinal fibrosis complicating healed primary histoplasmosis and tuberculosis. Medicine. 1972;51:227–46. - PubMed
-
- Peikert T, Colby TV, Midthun DE, et al. Fibrosing mediastinitis: Clinical presentation, therapeutic outcomes, and adaptive immune response. Medicine. 2011;90:412–23. - PubMed
-
- Rossi SE, McAdams HP, Rosado-de-Christenson ML, et al. Fibrosing mediastinitis. Radiographics. 2001;21:737–57. - PubMed
-
- Rossi GM, Emmi G, Corradi D, et al. Idiopathic mediastinal fibrosis: A systemic immune-mediated disorder. A case series and a review of the literature. Clinic Rev Allerg Immunol. 2017;52:446–59. - PubMed
-
- Lindholm KE, de Groot P, Moran CA. Fibrosing/sclerosing lesions of the mediastinum: A review. Adv Anat Pathol. 2019;26:235–40. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
