

Gallbladder perforation causing local peritonitis in left upper abdomen: A case report
- PMID: 39736245
- PMCID: PMC11743910
- DOI: 10.1016/j.ijscr.2024.110772
Gallbladder perforation causing local peritonitis in left upper abdomen: A case report
Abstract
Introduction and importance: Type 1 gallbladder perforation (GBP) in the free abdominal cavity causes pan-peritonitis, which is both rare and difficult to diagnose.
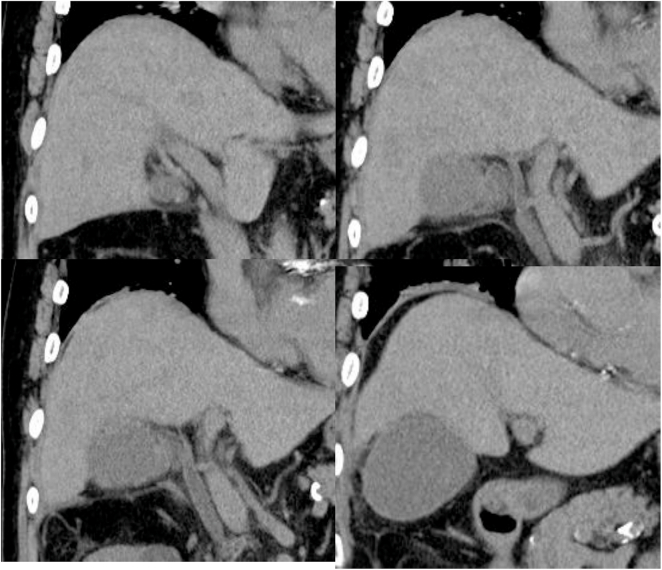
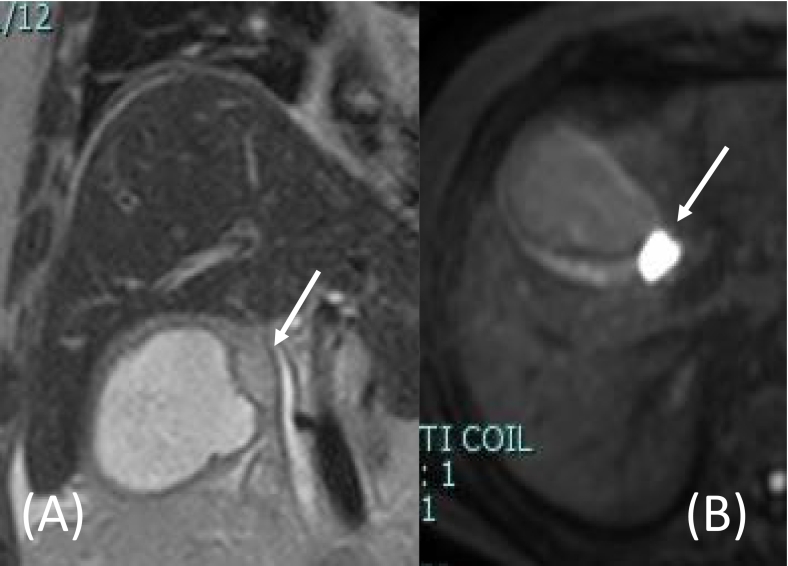
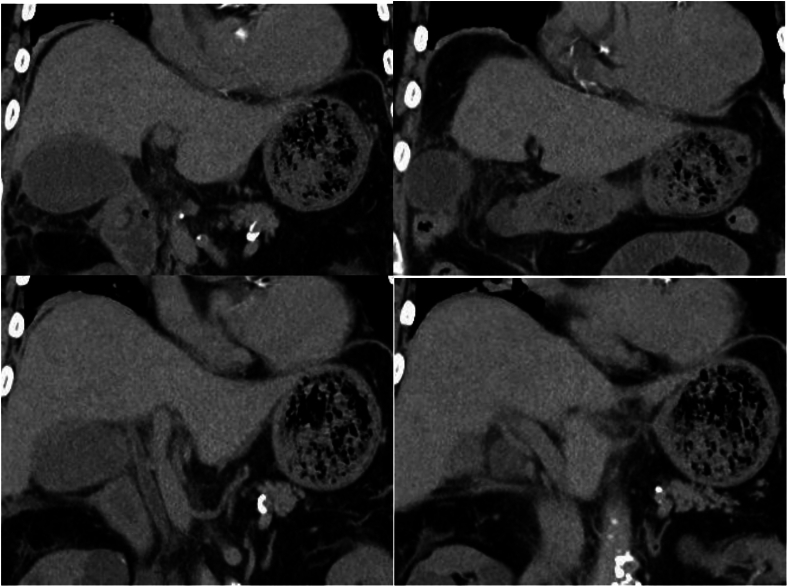
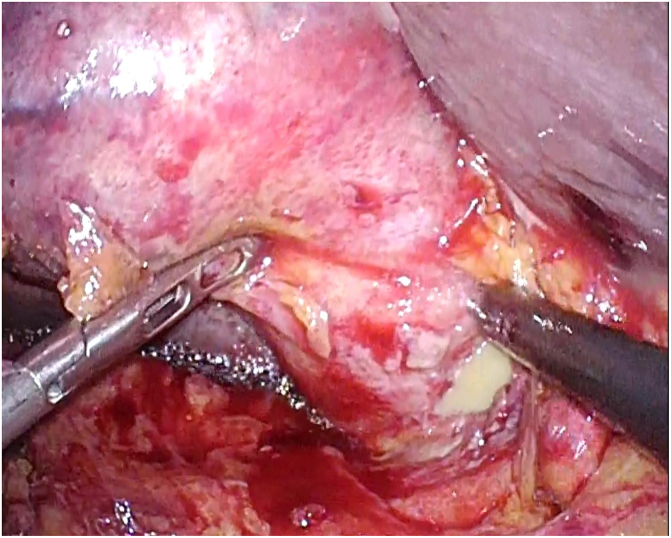
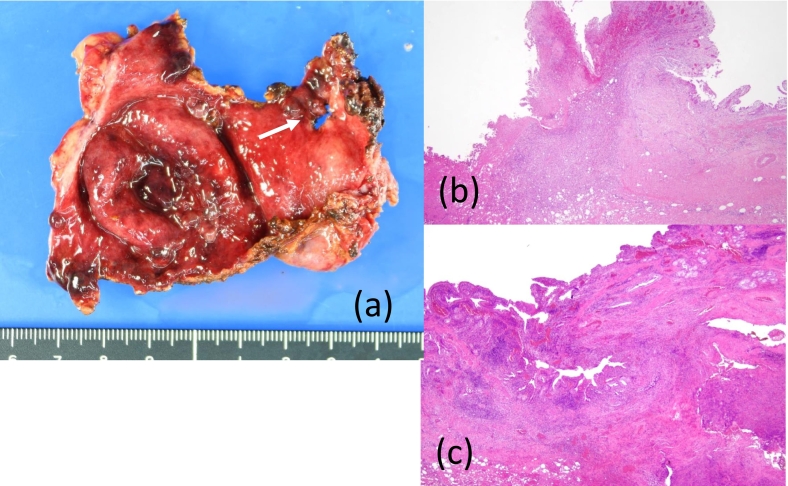
Case presentation: An 80-year-old man presented to our hospital with acute left upper abdominal pain. Twenty days prior to presentation, he had been admitted for 12 days with coronavirus disease 2019 (COVID-19). The patient had mild cholecystitis and received conservative therapy for COVID-19. Upon readmission, his abdomen was flat and soft except for local peritonitis in the left upper abdomen. An emergency laparoscopy revealed a perforation in the ventral wall of the gallbladder neck discharging pus under the lateral lobe of the liver without a gastrointestinal perforation. Therefore, a laparoscopic cholecystectomy and intra-abdominal lavage were performed. Based on the clinical and pathological findings, the GBP was suspected to be a rupture of the abscess in the Rokitansky-Aschoff sinus observed on magnetic resonance imaging during the first admission.
Discussion: In this case, acute cholecystitis was suppressed by conservative therapy, leaving adhesions of the surrounding tissue and viscus to the gallbladder fundus and body as well as an abscess in the wall of the neck. This was the cause of the GBP and resulted in local peritonitis within the left upper abdomen.
Conclusion: Type 1 GBP develops suddenly and cannot be predicted. In cases of acute cholecystitis once suppressed by conservative therapy and accompanied by cystic formation in the gallbladder wall, early cholecystectomy is recommended considering the risk of GBP.
Keywords: Acute cholecystitis; Covid-19; Exploratory laparoscopy; Laparoscopic cholecystectomy; Rokitansky-Aschoff sinus.
Copyright © 2024 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Conflict of interest statement There are no conflicts of interest.
Figures
Similar articles
-
Gallbladder perforation: A rare case report.Int J Surg Case Rep. 2023 Mar;104:107927. doi: 10.1016/j.ijscr.2023.107927. Epub 2023 Feb 11. Int J Surg Case Rep. 2023. PMID: 36791527 Free PMC article.
-
Laparoscopic Management of Spontaneous Gallbladder Perforation in Acalculous Cholecystitis: A Case Series.Cureus. 2024 Nov 13;16(11):e73587. doi: 10.7759/cureus.73587. eCollection 2024 Nov. Cureus. 2024. PMID: 39677234 Free PMC article.
-
Cholecysto-hepatic fistula in type III gallbladder perforation: A rare etiology of liver abscess; case report.Int J Surg Case Rep. 2023 Apr;105:108002. doi: 10.1016/j.ijscr.2023.108002. Epub 2023 Mar 23. Int J Surg Case Rep. 2023. PMID: 36965442 Free PMC article.
-
[Gallbladder volvulus: Diagnostic and surgical challenges].Cir Cir. 2017 Dec;85 Suppl 1:89-92. doi: 10.1016/j.circir.2016.10.013. Epub 2016 Dec 10. Cir Cir. 2017. PMID: 27955849 Review. Spanish.
-
Unusual case of Niemeier type II gallbladder perforation: case report and literature review.J Int Med Res. 2024 Jun;52(6):3000605241257452. doi: 10.1177/03000605241257452. J Int Med Res. 2024. PMID: 38835120 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
