

Fatigue, pain and faecal incontinence in adult inflammatory bowel disease patients and the unmet need: a national cross-sectional survey
- PMID: 39736517
- PMCID: PMC11686953
- DOI: 10.1186/s12876-024-03570-8
Fatigue, pain and faecal incontinence in adult inflammatory bowel disease patients and the unmet need: a national cross-sectional survey
Abstract
Background and aims: The co-existence of fatigue, pain and faecal incontinence in people with Inflammatory Bowel Disease (IBD) is unknown. We aimed to determine the presence of and relationship between these symptoms and patients' desire for intervention.
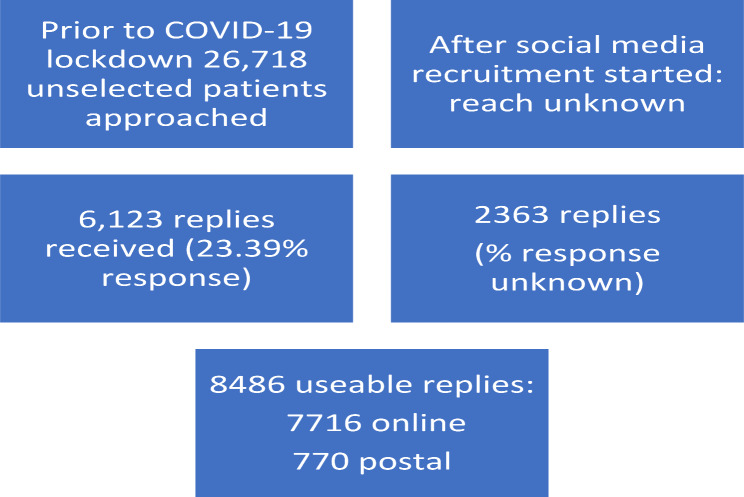
Methods: Adults with IBD in the UK, recruited from clinics, the national IBD-BioResource, a patient charity and social media sources, completed PROMIS validated patient-reported questionnaires to identify fatigue, pain and faecal incontinence, in addition to symptom severity and impact, disease activity, anxiety and depression questionnaires and questions about their desire for help with these symptoms. Statistical analysis used descriptive statistics to report presence of symptoms and Pearson correlation coefficients were calculated.
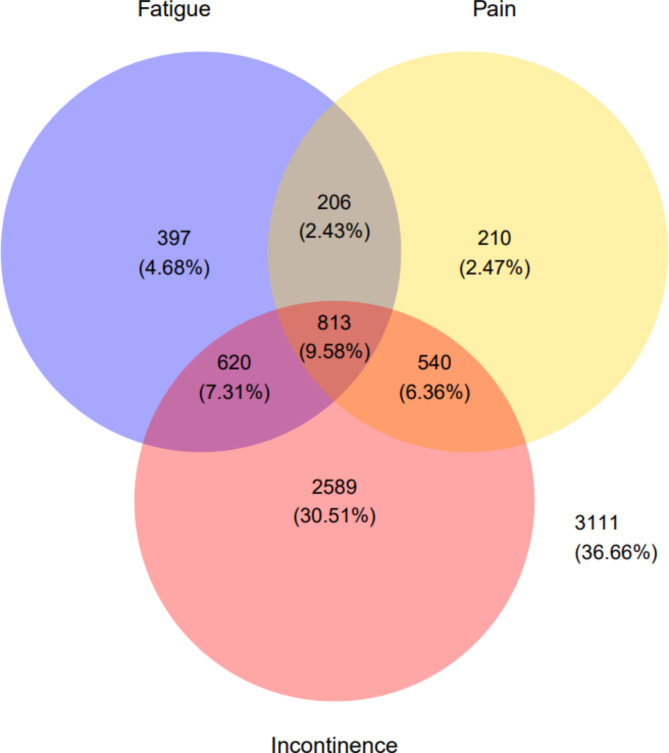
Results: Of 8486 responses, 54% reported faecal incontinence, 24% reported fatigue, and 21% reported pain; 10% reported all three symptoms in the past 7 days. Only 29% reported none of these symptoms. Fatigue and pain were moderately correlated (Pearson correlation coefficient 0.57); both fatigue and pain had a lower correlation with faecal incontinence (0.43 and 0.46 respectively). On a 0-10 scale for severity, participants scored fatigue highest, followed by incontinence then pain. For impact, participants scored incontinence highest, followed by fatigue then pain. 56% reported depression (27% with clinically relevant levels) and 49% reported anxiety (20% with clinically relevant levels); 23% had previously medically diagnosed mental health disorders. 56% of respondents "definitely" wanted help for fatigue; 53% for incontinence; 42% for pain; 29% "definitely" wanted help with all three symptoms. Factors associated with all three symptoms were Crohn's disease (vs. ulcerative colitis), IBD activity, IBD Control score, anxiety, depression, and history of surgery (all p ≤ 0.0001).
Conclusions: Fatigue, pain and incontinence are common in IBD and patients desire help for these symptoms, currently a substantial unmet need. Anxiety and depression are common, are underdiagnosed, and are independently associated with these symptoms.
Keywords: Crohn’s disease; Faecal incontinence; Fatigue; Inflammatory bowel disease; Pain; Ulcerative colitis.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethics approval was received from North West - Greater Manchester West Research Ethics Committee (Reference no: 18/NW/0613) on 11th October 2018. Informed consent to participate was obtained from all participants either in writing (postal) or online before accessing the online version of the survey. The study conformed to the requirements of the Helsinki declaration and the principles of Good Clinical Practice (GCP). Consent for publication: Not applicable. Competing interests: Ailsa Hart: has served as consultant, advisory board member or speaker for AbbVie, Arena, Atlantic, Bristol-Myers Squibb, Celgene, Celltrion, Falk, Galapogos, Lilly, Janssen, MSD, Napp Pharmaceuticals, Pfizer, Pharmacosmos, Shire and Takeda. She also serves on the Global Steering Committee for Genentech.Laura Miller: NoneFionn Cléirigh Büttner: None.Thomas Hamborg: NoneSonia Saxena: is an NIHR Senior investigator, funded by the National Institute for Health Research (NIHR) School for Public Health Research Grant Reference Number NIHR 204000 and NIHR Northwest London Applied Research CollaborationRichard Pollok: has served as consultant, advisory board member, speaker and/or received educational grants from Dr Falk, Pharmacosmos, Takeda, Janssen, Napp pharmaceuticals and Ferring pharmaceuticals.Imogen Stagg: NoneVari Wileman: NoneQasim Aziz: Funding as PI from Classado Biosciences Ltd; Takeda Pharmaceuticals and Dr Falk Pharma UK for commercial clinical trials. Wladyslawa Czuber-Dochan: Speaker fees from Dr Falk Pharma and research funding from Bristol Myers Squibb and Crohn’s and Colitis UKLesley Dibley: funding to support research from Takeda, Janssen; speaker fees from Abbvie, Janssen and WedMD. BRUK advisory board. Borislava Mihaylova: None Rona Moss-Morris: NoneChris Roukas: NoneChristine Norton: Speaker fees from: Janssen, WebMD, Medscape, Merck Pharmaceutical; Tillotts Pharma UK. Pfizer advisory board.
Figures

Similar articles
-
Impact of pain, fatigue and bowel incontinence on the quality of life of people living with inflammatory bowel disease: A UK cross-sectional survey.United European Gastroenterol J. 2025 Apr;13(3):364-375. doi: 10.1002/ueg2.12668. Epub 2024 Oct 19. United European Gastroenterol J. 2025. PMID: 39425758 Free PMC article.
-
Impacts of perianal disease and faecal incontinence on quality of life and employment in 1092 patients with inflammatory bowel disease.Aliment Pharmacol Ther. 2018 May;47(9):1253-1260. doi: 10.1111/apt.14599. Epub 2018 Mar 9. Aliment Pharmacol Ther. 2018. PMID: 29520808 Free PMC article.
-
Supported online self-management versus care as usual for symptoms of fatigue, pain and urgency/incontinence in adults with inflammatory bowel disease (IBD-BOOST): study protocol for a randomised controlled trial.Trials. 2021 Aug 3;22(1):516. doi: 10.1186/s13063-021-05466-4. Trials. 2021. PMID: 34344432 Free PMC article.
-
Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: a systematic review and meta-analysis.Lancet Gastroenterol Hepatol. 2021 May;6(5):359-370. doi: 10.1016/S2468-1253(21)00014-5. Epub 2021 Mar 12. Lancet Gastroenterol Hepatol. 2021. PMID: 33721557
-
Targets for interventions for faecal incontinence in inflammatory bowel disease: a systematic review.Scand J Gastroenterol. 2018 Dec;53(12):1476-1483. doi: 10.1080/00365521.2018.1543451. Epub 2019 Jan 22. Scand J Gastroenterol. 2018. PMID: 30668177
Cited by
-
Care needs profiles of Crohn's disease patients and their associations with symptom clusters, post-traumatic growth, and family function: a latent profile analysis.BMC Gastroenterol. 2025 May 9;25(1):351. doi: 10.1186/s12876-025-03953-5. BMC Gastroenterol. 2025. PMID: 40346452 Free PMC article.
-
What is the impact on recruitment of a shortened compared with a standard-length participant information leaflet? PROMETHEUS in IBD-BOOST: study within a trial, a decentralised UK randomised controlled trial.Trials. 2025 Jun 18;26(1):211. doi: 10.1186/s13063-025-08931-6. Trials. 2025. PMID: 40528252 Free PMC article. Clinical Trial.
References
-
- Wilson BS, Lonnfors S, Vermeire S, Greco M, Hommes DW, Bell C et al. The true impact of IBD: a European Crohn’s and Ulcerative Colitis patient life impact survey 2010-11. 2012 2012.
-
- Proudfoot H, Norton C, Artom M, Didymus E, Kubasiewicz S, Khoshaba K. Systematic review: targets for health interventions for faecal incontinence in inflammatory bowel disease. Scand J Gastroenterol. 2018;53(12):1476–83. - PubMed
-
- Artom M, Czuber-Dochan W, Sturt J, Norton C. Targets for health interventions for inflammatory bowel disease-fatigue. J Crohn’s Colitis. 2016;10(7):860–9. - PubMed
-
- Sweeney L, Moss-Morris R, Czuber-Dochan W, Meade L, Chumbley G, Norton C. Systematic review: psychosocial factors associated with pain in inflammatory bowel disease. Aliment Pharmacol Ther. 2018;47:715–29. - PubMed
-
- Norton C, Dibley L. Help-seeking for fecal incontinence in people with inflammatory bowel disease. J Wound Ostomy Cont Nurs. 2013;40(6):631–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
