

Age, frequency, and strategy optimization for organized colorectal cancer screening: a decision analysis conducted in China for the years 2023-2038
- PMID: 39736566
- PMCID: PMC11686884
- DOI: 10.1186/s12885-024-13319-x
Age, frequency, and strategy optimization for organized colorectal cancer screening: a decision analysis conducted in China for the years 2023-2038
Abstract
Background: The colorectal cancer mortality rate in China has exceeded that in many developing countries and is expected to further increase owing to multiple factors, including the aging population. However, the optimal policy for colorectal cancer screening is unknown.
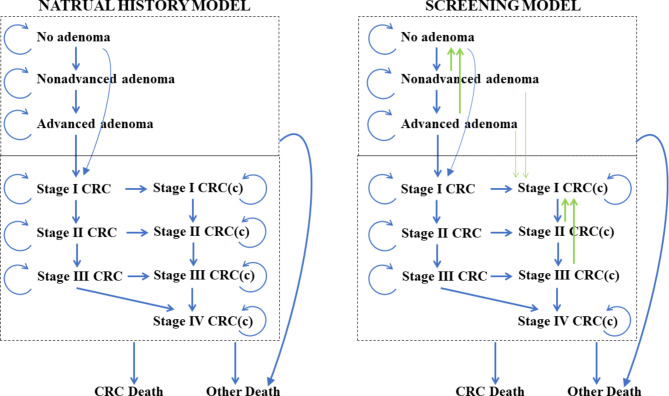
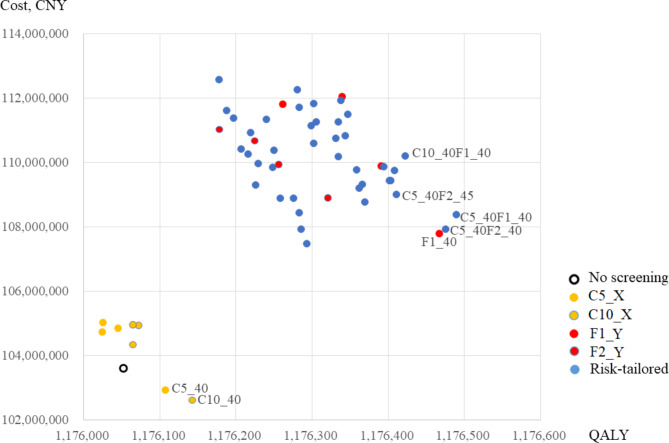
Methods: We synthesized the most up-to-date data using a 12-state Markov model populated with a cohort of Chinese men and women born during 1949-1988, and evaluated 16 conventional and 40 risk-tailored schemes for colorectal cancer screening, considering possible combinations of age (starting at 40 + years and ending at 75 years), frequency, and strategy (standard colonoscopy, fecal immunochemical testing with colonoscopy if positive, or risk-tailored). We projected the incidence and mortality of CRC, cost, and quality-adjusted life years for 2023-2038; and performed incremental cost-effectiveness, probability acceptability, and sensitivity analyses to identify the optimal scheme and the factors affecting this choice.
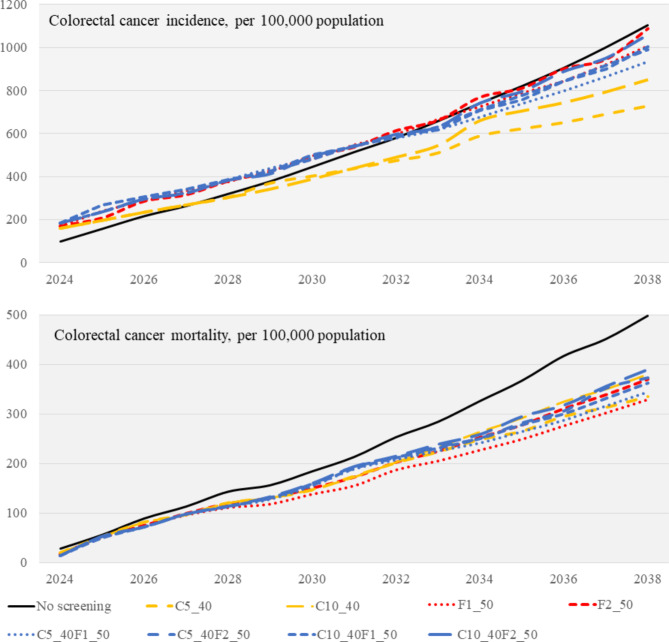
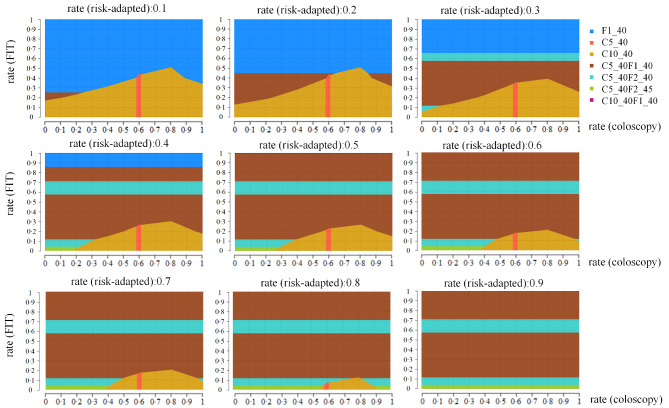
Results: By 2038, all standard colonoscopy, colonoscopy following fecal immunochemical testing, and risk-tailored schemes were effective in reshaping China's colorectal cancer trajectory, with relative reductions in colorectal cancer incidence and mortality rates of up to 34% and 33.7%, respectively, versus no screening. Two standard colonoscopy, one colonoscopy following fecal immunochemical testing, and four risk-tailored schemes were efficient using a starting age of 40 years. Among these options, a risk-tailored scheme (standard colonoscopy every 5 years for high-risk and annual fecal immunochemical testing screening for moderate-to-low-risk) had a high probability (31.1%) of being optimal (with ≥ 40% uptake for a high-risk population, in particular), given China's present per capita gross domestic product, and would yield the highest gain in quality-adjusted life years in 17 of 31 provinces.
Conclusions: Our findings suggest the commencement of colorectal cancer screening at 40 years of age in China, and that risk-tailored and some conventional schemes would be effective and cost-efficient. These findings should be valuable for policy-making regarding cancer control and resource allocation.
Keywords: Cancer screening; Colorectal cancer; Cost effectiveness; Decision analysis; Early onset.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Cost-effectiveness and budget impact analyses of colorectal cancer screenings in a low- and middle-income country: example from Thailand.J Med Econ. 2019 Dec;22(12):1351-1361. doi: 10.1080/13696998.2019.1674065. Epub 2019 Oct 12. J Med Econ. 2019. PMID: 31560247
-
Clinical and Economic Impact of Tailoring Screening to Predicted Colorectal Cancer Risk: A Decision Analytic Modeling Study.Cancer Epidemiol Biomarkers Prev. 2020 Feb;29(2):318-328. doi: 10.1158/1055-9965.EPI-19-0949. Epub 2019 Dec 3. Cancer Epidemiol Biomarkers Prev. 2020. PMID: 31796524
-
Optimal use of colonoscopy and fecal immunochemical test for population-based colorectal cancer screening: a cost-effectiveness analysis using Japanese data.Jpn J Clin Oncol. 2016 Feb;46(2):116-25. doi: 10.1093/jjco/hyv186. Epub 2015 Dec 18. Jpn J Clin Oncol. 2016. PMID: 26685321
-
Cost-Effectiveness of Current Colorectal Cancer Screening Tests.Gastrointest Endosc Clin N Am. 2020 Jul;30(3):479-497. doi: 10.1016/j.giec.2020.02.005. Epub 2020 Apr 9. Gastrointest Endosc Clin N Am. 2020. PMID: 32439083 Review.
-
Efficacy and cost-effectiveness of fecal immunochemical test versus colonoscopy in colorectal cancer screening: a systematic review and meta-analysis.Gastrointest Endosc. 2020 Mar;91(3):684-697.e15. doi: 10.1016/j.gie.2019.11.035. Epub 2019 Nov 30. Gastrointest Endosc. 2020. PMID: 31790657
Cited by
-
An insight into the role of innate immune cells in breast tumor microenvironment.Breast Cancer. 2025 Jan;32(1):79-100. doi: 10.1007/s12282-024-01645-8. Epub 2024 Oct 26. Breast Cancer. 2025. PMID: 39460874 Review.
-
Colonic Aging and Colorectal Cancer: An Unignorable Interplay and Its Translational Implications.Biology (Basel). 2025 Jul 3;14(7):805. doi: 10.3390/biology14070805. Biology (Basel). 2025. PMID: 40723364 Free PMC article. Review.
References
-
- International Agency for Research on Cancer. Global cancer observatory. https://gco.iarc.fr/today/. Accessed 15 Oct 2023.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
