

Locking compression plate as a sequential external fixator following the distraction phase for the treatment of tibial bone defects caused by fracture-related infection: experiences from 22 cases
- PMID: 39736587
- PMCID: PMC11684307
- DOI: 10.1186/s12891-024-08221-3
Locking compression plate as a sequential external fixator following the distraction phase for the treatment of tibial bone defects caused by fracture-related infection: experiences from 22 cases
Abstract
Background: The purpose of this study was to report the clinical and psychological outcomes of using a locking compression plate (LCP) as a sequential external fixator following the distraction phase in the treatment of tibial bone defects caused by fracture-related infection (FRI).
Methods: We retrospectively analyzed the clinical records and consecutive X-ray images of patients with tibial bone defects who were treated with an LCP as a sequential external fixator following the distraction phase, between June 2017 and December 2022. The ASAMI criteria were applied to assess the bone and functional outcomes, and postoperative complications were evaluated by using the Paley classification. The SCL-90-R questionnaire was used to evaluate patients' psychological symptoms, documented and compared at Time 1 (before bone transport), Time 2 (after distraction phase), and Time 3(final follow-up). Statistical significance was set at P < 0.05.
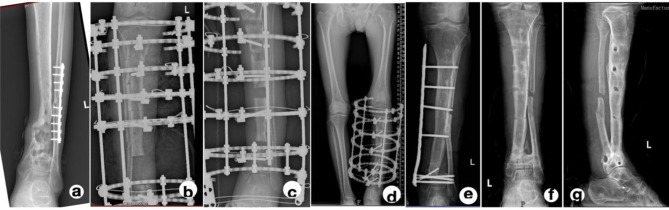
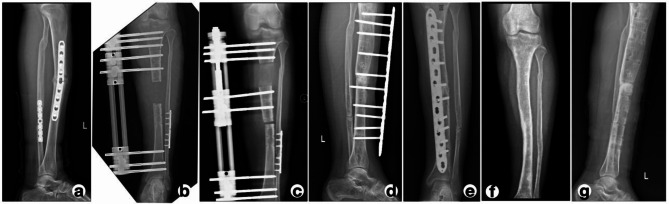
Results: This study included 22 participants with a mean age of 37.72 ± 9.65 years, comprising 17 males (77.2%) and 5 females (22.7%). The mean postoperative follow-up time was 29 ± 2.65 months. The mean number of previous surgical interventions per patient was 5.22 ± 1.26. Twenty-two patients with tibial bone defects caused by FRI were successfully treated using an LCP as a sequential external fixator following the distraction phase, with a mean bone union time of 9.95 ± 1.52 months. Bone union was achieved in all cases (100%) without the use of bone grafts at the docking sites. Following the completion of distraction, the Ilizarov apparatus or monorail fixator was retained for an additional 2.20 ± 0.53 weeks before being exchanged for the external locking compression plate (ELCP). The mean external fixation time (EFT) was 12.29 ± 1.67 months, with a mean external fixation index (EFI) of 1.83 ± 0.22 month/cm (Table 2). At the final follow-up, bone and functional outcomes were evaluated using the ASAMI criteria. Bone outcomes included 10 excellent and 12 good results, while functional outcomes included 12 excellent, 9 good, and 1 fair result. Statistically significant differences in psychological impacts were observed among the three time points (Time 1 vs. Time 2, P = 0.034; Time 2 vs. Time 3, P = 0.020; Time 1 vs. Time 3, P = 0.012). Complications were observed in 6 patients (27.2%), including joint stiffness (n = 3), pin-track infection (n = 3), and refracture (n = 1). All complications were successfully managed.
Conclusion: LCP used as a sequential external fixator following the distraction phase is an effective method for treating massive tibial bone defects caused by FRI and is also suitable for patients with scars and poor tissue conditions resulting from multiple previous debridement. Furthermore, this combined technique could be more beneficial in alleviating psychological burdens, supporting patients' engagement in rehabilitation, and facilitating a return to normal life.
Clinical trial number: Not applicable.
Keywords: Bone defect; External fixation; Ilizarov bone transport; Locking compression plate; Tibia.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This retrospective study was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University and carried out by the ethical standards set out in the Helsinki Declaration. Informed consent was received from all participants. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Bezstarosti H, Metsemakers WJ, van Lieshout EMM, Voskamp LW, Kortram K, McNally MA, Marais LC, Verhofstad MHJ. Management of critical-sized bone defects in the treatment of fracture-related infection: a systematic review and pooled analysis. Arch Orthop Trauma Surg. 2021;141(7):1215–30. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
