

A new distal radius fracture classification depending on the specific fragments through machine learning clustering method
- PMID: 39736589
- PMCID: PMC11684110
- DOI: 10.1186/s12891-024-08215-1
A new distal radius fracture classification depending on the specific fragments through machine learning clustering method
Abstract
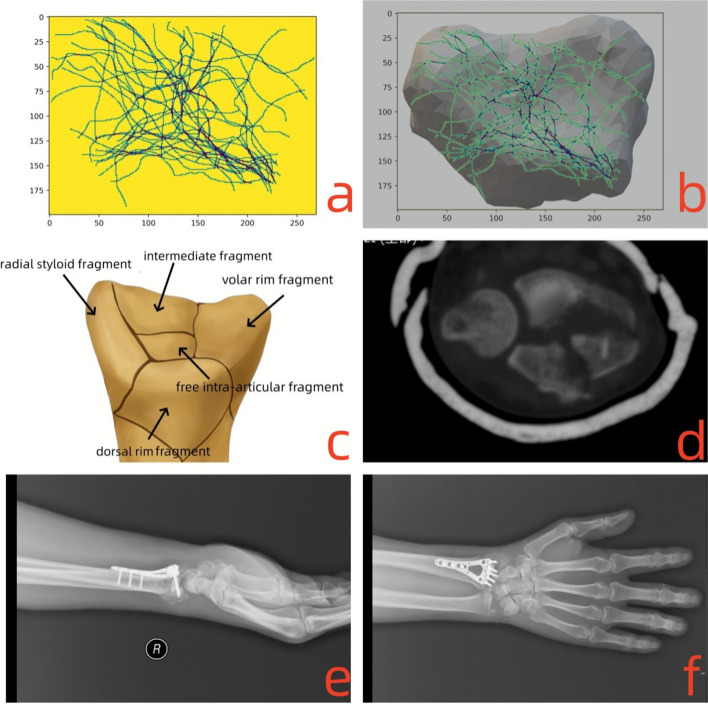
Purposes: The objective of this study was to investigate intra-articular distal radius fractures, aiming to provide a comprehensive analysis of fracture patterns and discuss the corresponding treatment strategies for each pattern.
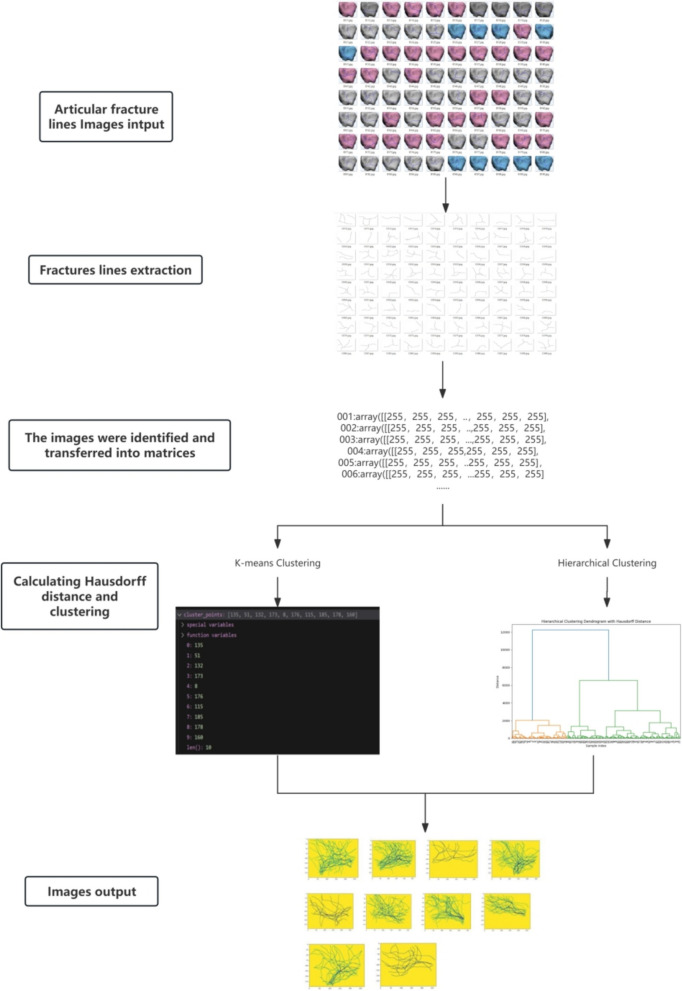
Methods: 294 cases of intra-articular distal radius fractures lines were collected and clustered thorough K-means and hierarchical clustering algorithm. The demographic data of patients and the clinical treatment outcomes were recorded. For functional evaluation, quick Disabilities of the Arm, Shoulder, and Hand (DASH) score, visual analog scale (VAS) pain score, range of motion (ROM) of the wrist joint and the percentage of the grip strength relative to the healthy wrist at 12 months follow-up were evaluated and recorded; For radiographic parameters of volar tilt (VT), radial inclination (RI), and ulnar variance (UV) were obtained; The occurrence of complications was carefully assessed and documented.
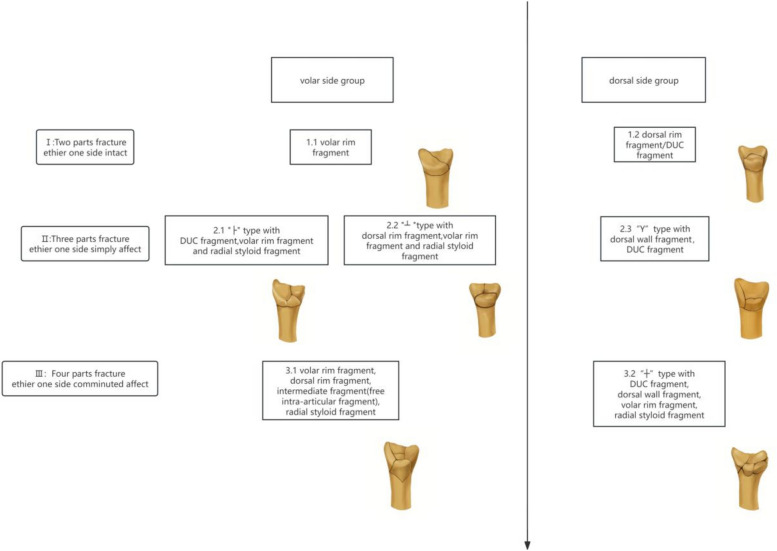
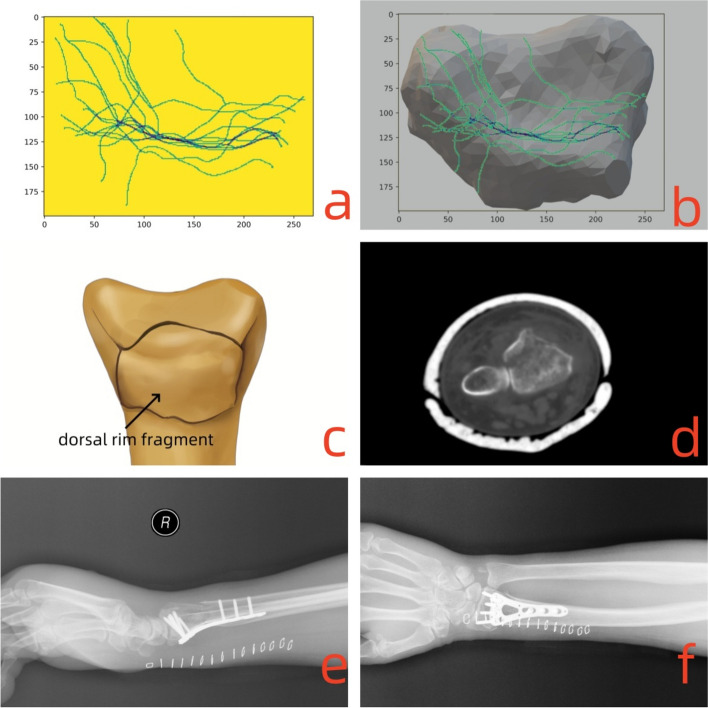
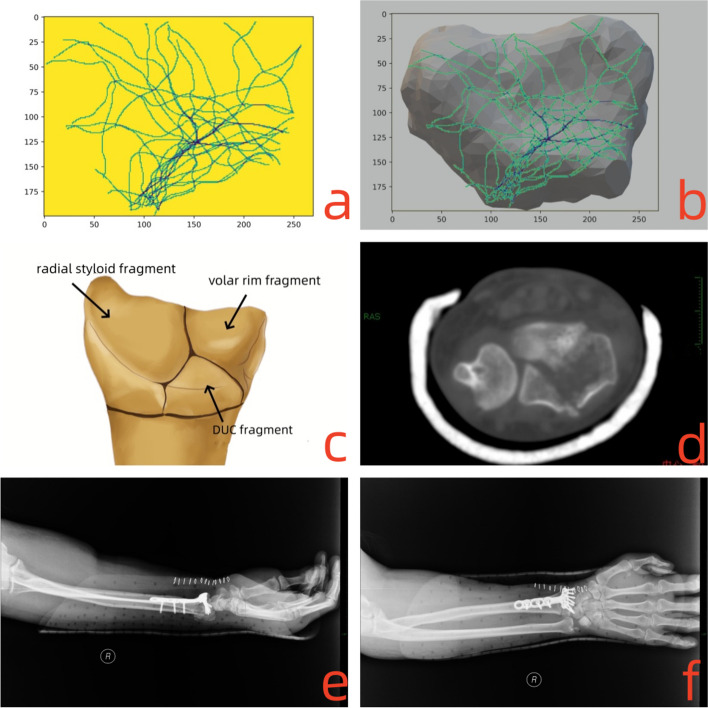
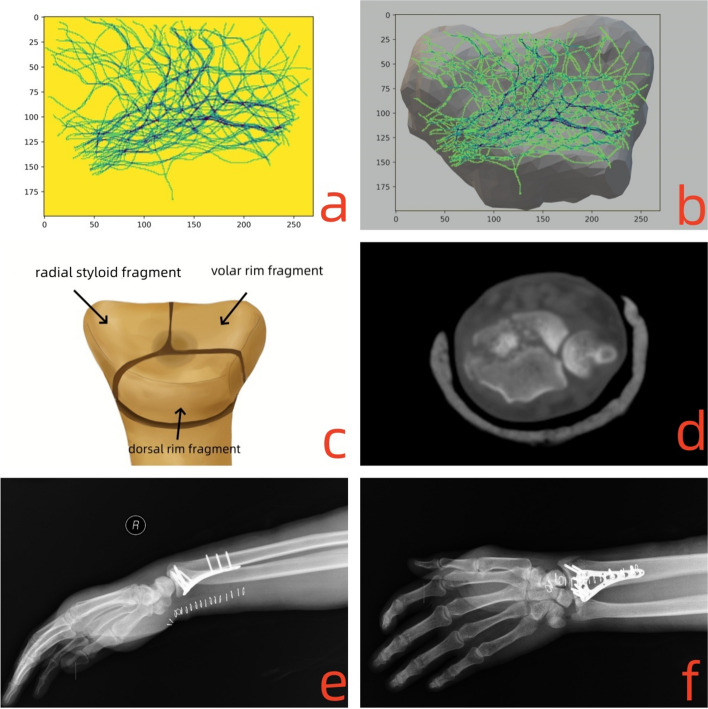
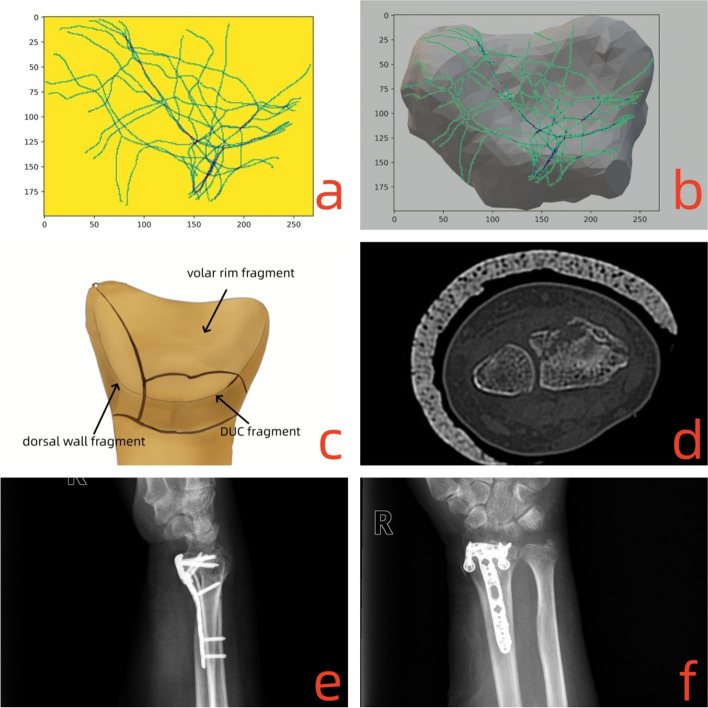
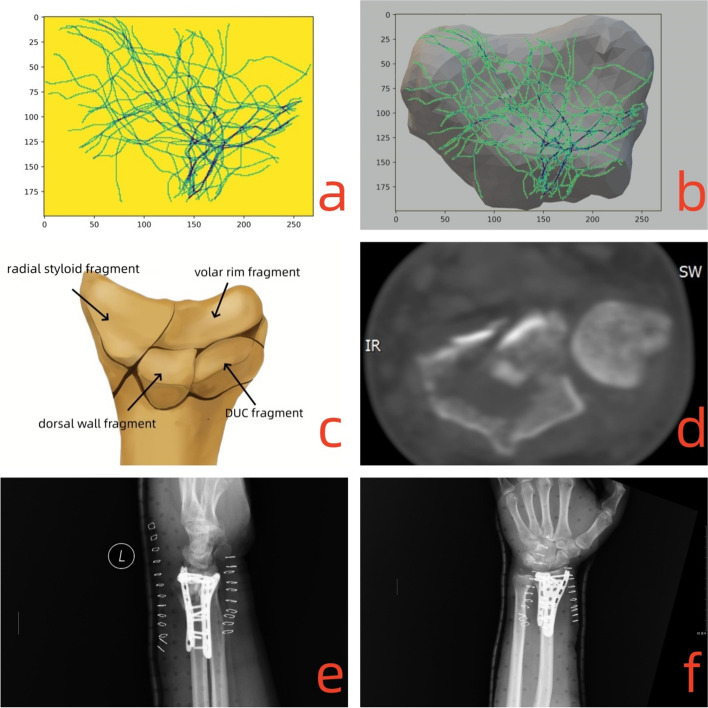
Results: Totally 294 patients were included and divided into the volar side affected group and the dorsal side affected groups. And each group was further categorized into three types: type I, with two parts fractures with either one volar/dorsal side intact; type II, with three parts fractures with volar/dorsal side simply affected; and type III, with four parts fractures with volar/dorsal side communited affected. The volar plate fixation was performed as the standard treatment, while the combined plate fixation was used for comminuted dorsal bone defects of the metaphysis and impaction. There were no differences in the postoperative radiograph parameters, functional outcomes and incidences of complications for each type of volar side group and dorsal side group except that the 3.2 type DRFs showed less range of flexion (75.56±7.48)° and extension (61.65±9.9)° than other dorsal types.
Conclusions: A new intra-articular distal radius fractures classification was proposed based on the affection condition of volar or dorsal side. The volar plate fixation is an effective treatment for the intra-articular distal radius fractures, while combined plate fixation can be considered as an alternative treatment for dorsal side comminuted fractures.
Level of evidence: III a.
Keywords: Articular; Classification; Combined fixation; Distal radius fractures; Machine learning; Plate fixation; Specific fragment.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Ethics Committee of Chaoyang Hospital, Capital Medical University in accordance with the Declaration of Helsinki.(Clinical trial number :2021-科-441;Registration Date: 2021/7/5) Informed consent to participate was obtained from all of the participants in the study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Comparison between Carbon-Peek volar locking plates and titanium volar locking plates in the treatment of distal radius fractures.Injury. 2017 Oct;48 Suppl 3:S24-S29. doi: 10.1016/S0020-1383(17)30653-8. Injury. 2017. PMID: 29025605 Clinical Trial.
-
Corrective Osteotomy with Volar and Dorsal Fixation for Malunion of Intra-Articular Fracture of the Distal Radius: A Retrospective Study.Orthop Surg. 2022 Aug;14(8):1751-1758. doi: 10.1111/os.13409. Epub 2022 Jul 22. Orthop Surg. 2022. PMID: 35866348 Free PMC article.
-
Is it really necessary to restore radial anatomic parameters after distal radius fractures?Injury. 2014 Dec;45 Suppl 6:S21-6. doi: 10.1016/j.injury.2014.10.018. Epub 2014 Oct 27. Injury. 2014. PMID: 25457314 Review.
-
Functional outcome of unstable distal radius fractures: ORIF with a volar fixed-angle tine plate versus external fixation.J Hand Surg Am. 2005 Mar;30(2):289-99. doi: 10.1016/j.jhsa.2004.11.014. J Hand Surg Am. 2005. PMID: 15781351
-
The use of dorsal distraction plating for severely comminuted distal radius fractures: A review and comparison to volar plate fixation.Injury. 2019 Jun;50 Suppl 1:S50-S55. doi: 10.1016/j.injury.2019.03.052. Epub 2019 Apr 6. Injury. 2019. PMID: 31040029 Review.
References
-
- Constant CR, Gerber C, Emery RJ, Søjbjerg JO, Gohlke F, Boileau P. A review of the constant score: modifications and guidelines for its use. J Shoulder Elb Surg. 2008;17(2):355–61. 10.1016/j.jse.2007.06.022. - PubMed
-
- Cooney WP 3rd, Linscheid RL, Dobyns JH. External pin fixation for unstable Colles’ fractures. J Bone Joint Surg Am. 1979;61(6A):840–5. - PubMed
-
- Leung KS, Shen WY, Tsang HK, Chiu KH, Leung PC, Hung LK. An effective treatment of comminuted fractures of the distal radius. J Hand Surg Am. 1990;15(1):11–7. 10.1016/s0363-5023(09)91098-x. - PubMed
-
- Mandziak DG, Watts AC, Bain GI. Ligament contribution to patterns of articular fractures of the distal radius. J Hand Surg Am. 2011;36(10):1621–5. 10.1016/j.jhsa.2011.07.014. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
