

Surgical delay-associated mortality risk varies by subtype in loco-regional breast cancer patients in SEER-Medicare
- PMID: 39736650
- PMCID: PMC11686992
- DOI: 10.1186/s13058-024-01949-9
Surgical delay-associated mortality risk varies by subtype in loco-regional breast cancer patients in SEER-Medicare
Abstract
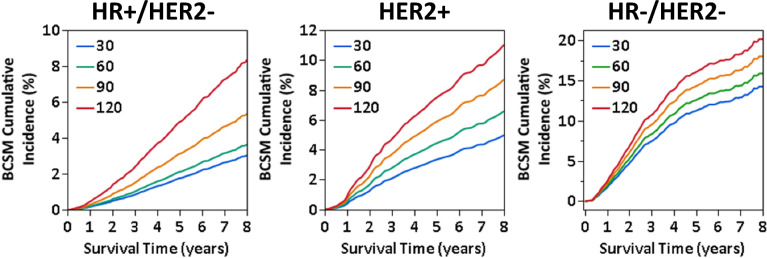
Substantial evidence supports that delay of surgery after breast cancer diagnosis is associated with increased mortality risk, leading to the introduction of a new Commission on Cancer quality measure for receipt of surgery within 60 days of diagnosis for non-neoadjuvant patients. Breast cancer subtype is a critical prognostic factor and determines treatment options; however, it remains unknown whether surgical delay-associated breast cancer-specific mortality (BCSM) risk differs by subtype. This retrospective cohort study aimed to assess whether the impact of delayed surgery on survival varies by subtype (hormone [HR] + /HER2 -, HR -/HER2 -, and HER2 +) in patients with loco-regional breast cancer who received surgery as their first treatment between 2010 and 2017 using the SEER-Medicare database. Exposure of this study was continuous time to surgery from diagnostic biopsy (TTS; days) in reference to TTS = 30 days. BCSM were evaluated as flexibly dependent on continuous time (days) to surgery from diagnosis (TTS) using Fine and Gray competing-risk regression models, respectively, by HR status. Inverse propensity score-weighting was adjusted for demographic, clinical, and treatment variables impacting TTS. Adjusted BCSM risk grew with increasing TTS across all subtypes; however, the pattern and extent of the association varied. HR + /HER2 - patients exhibited the most pronounced increase in BCSM risk associated with TTS, with approximately exponential growth after 42 days, with adjusted subdistribution hazard ratios (sHR) of 1.21 (95% CI: 1.06-1.37) at TTS = 60 days, 1.79 (95% CI: 1.40-2.29) at TTS = 90 days, and 2.83 (95% CI: 1.76-4.55) at TTS = 120 days. In contrast, both HER2 + and HR -/HER2 - patients showed slower, approximately linear growth in sHR, although non-significant in HR -HER2 -.
Keywords: Breast cancer-specific mortality; HER2; Hormone-receptor; SEER-Medicare; Surgical delay; Tumor subtype.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


Update of
-
Surgical Delay-Associated Mortality Risk Varies by Subtype in Loco-Regional Breast Cancer Patients in SEER-Medicare.Res Sq [Preprint]. 2024 Apr 8:rs.3.rs-4171651. doi: 10.21203/rs.3.rs-4171651/v1. Res Sq. 2024. Update in: Breast Cancer Res. 2024 Dec 30;26(1):191. doi: 10.1186/s13058-024-01949-9. PMID: 38659868 Free PMC article. Updated. Preprint.
References
-
- Breastcancer.org. Breast Cancer Facts and Statistics. 2024. https://www.breastcancer.org/facts-statistics
-
- Society AC. Breast cancer facts & figures 2024–2025. American Cancer Society 2024. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-...
-
- Early Breast Cancer Trialists' Collaborative G, Davies C, Godwin J, et al. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet. 2011;378(9793):771–84. 10.1016/S0140-6736(11)60993-8 - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
