

Impaired pulmonary function increases the risk of gout: evidence from a large cohort study in the UK Biobank
- PMID: 39736738
- PMCID: PMC11686989
- DOI: 10.1186/s12916-024-03836-8
Impaired pulmonary function increases the risk of gout: evidence from a large cohort study in the UK Biobank
Abstract
Background: Pulmonary function is increasingly recognized as a key factor in metabolic diseases. However, its link to gout risk remains unclear. The study aimed to investigate the relationship between pulmonary function and the risk of developing gout and the underlying biological mechanisms.
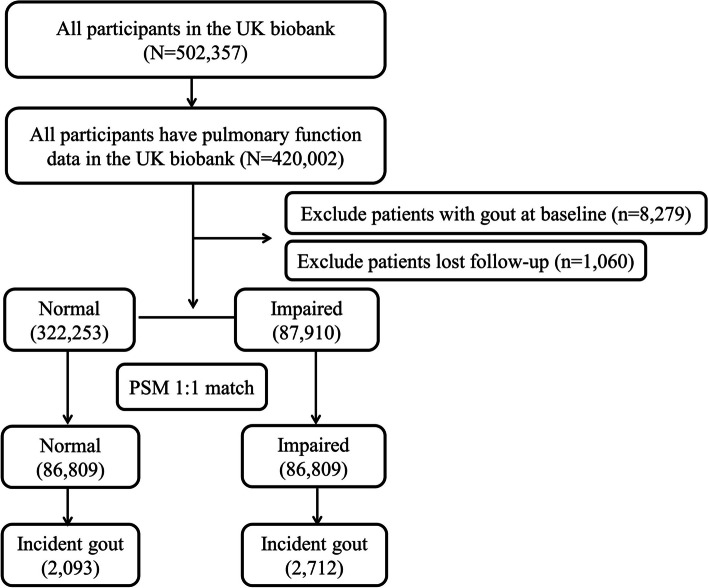
Methods: Our study included 420,002 participants with complete pulmonary function data from the UK Biobank. Logistic regression was used to evaluate gout prevalence among individuals with different pulmonary function statuses. Propensity score matching (PSM) created balanced groups, while Cox regression gauged the risk association between reduced lung capacity and gout compared with normal function. Mendelian randomization (MR) analysis was used to verify causal associations. Non-linear correlations were assessed with restricted cubic spline (RCS) analysis, and mediation analysis was used to explore the role of blood biomarkers. Mediation analyses were used to investigate the potential mediating role of biomarkers in the association.
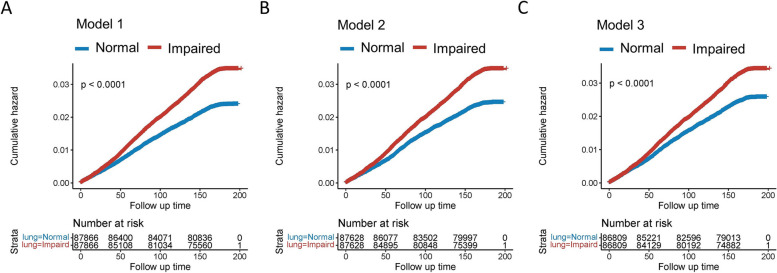
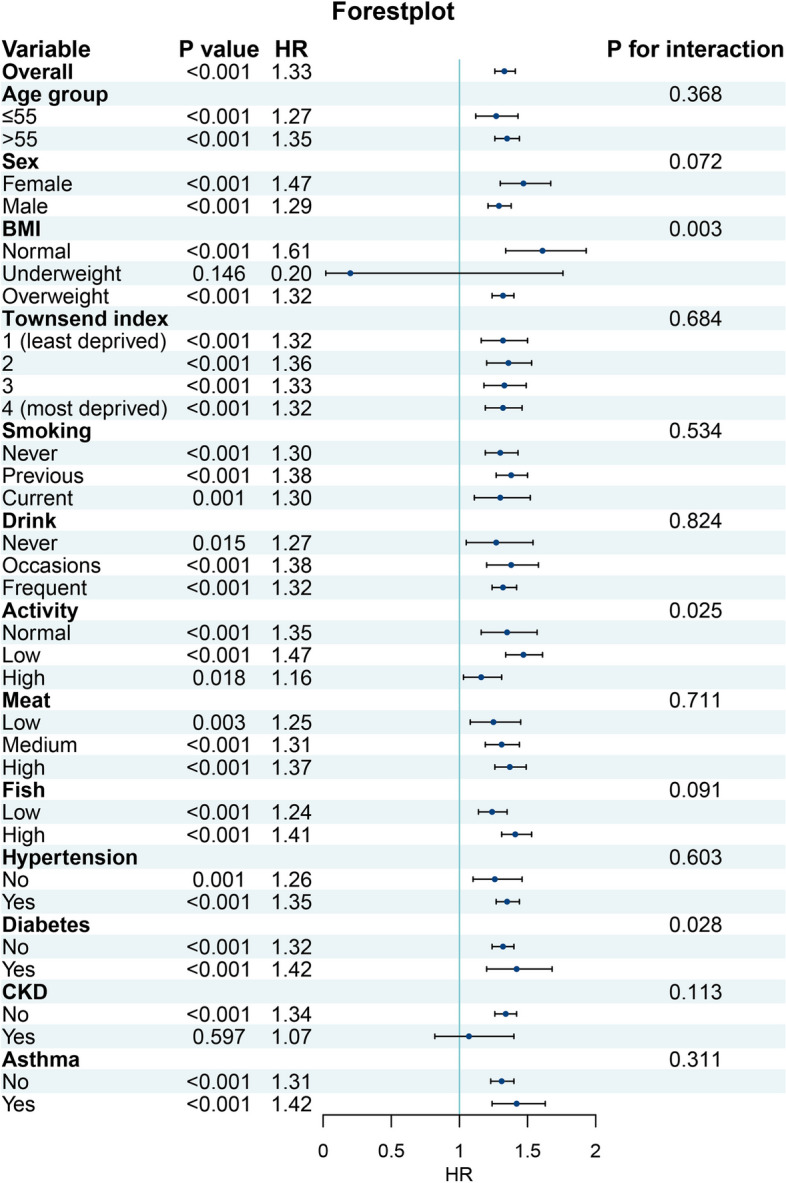
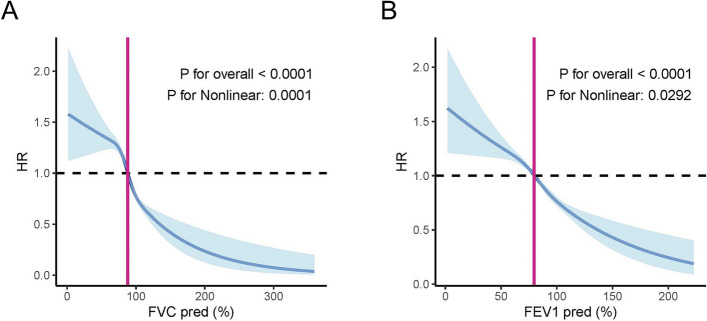
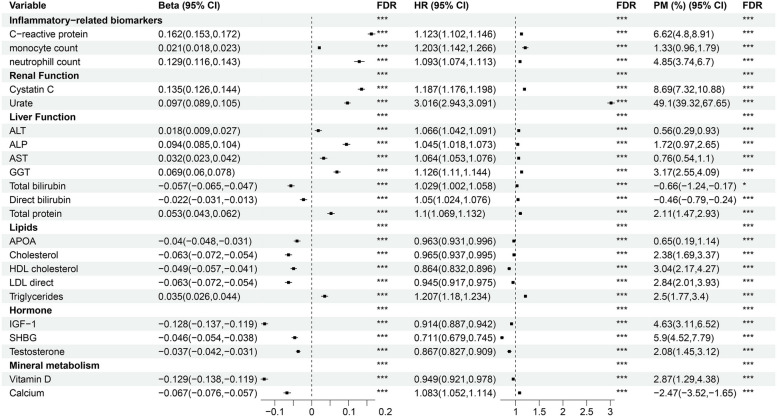
Results: Cross-sectional analysis revealed a higher prevalence of gout in individuals with preserved ratio of impaired spirometry (PRISm) of 6.31% and chronic obstructive pulmonary disease (COPD) of 6.26% than in those with normal pulmonary function (3.45%). After adjustment for covariates, both PRISm (odds ratio [OR] 1.24, 95% confidence interval [CI] 1.17-1.31) and COPD (OR 1.14, 95% CI 1.07-1.22) were significantly associated with gout. Longitudinal analysis confirmed that impaired pulmonary function significantly increased the risk of developing gout (hazard ratio [HR] 1.32, 95% CI 1.24-1.40). MR further revealed a potential causal effect of decreased pulmonary function on an increased risk of gout. Subgroup analysis revealed significant interactions between impaired pulmonary function and several factors, including body mass index (BMI), levels of physical activity, and diabetes status, in their associations with the risk of gout. RCS analysis showed a nonlinear relationship between pulmonary function indicators and gout incidence, characterized by an inverse S-shaped curve. Mediation analysis revealed that urate levels (49.1% mediation proportion), C-reactive protein (CRP) levels (6.62%), monocyte counts (1.33%), and neutrophil counts (4.85%) significantly mediated the relationship between pulmonary function and the risk of gout.
Conclusions: Our study revealed a significant association between impaired pulmonary function and an increased risk of developing gout. The association might be partially mediated by biomarkers including urate levels, inflammatory markers, and immune cell counts.
Keywords: Gout; Immune cell counts; Inflammation; Mediation analysis; Pulmonary function; Spirometry; UK Biobank; Urate levels.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The UK Biobank has obtained ethical approval from the North West Multi-centre Research Ethics Committee (Reference number: 11/NW/0382, https://www.ukbiobank.ac.uk/learn-more-about-uk-biobank/about-us/ethics ). Informed consent was collected from all study participants via electronic signature. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Prevalence, risk factors, and clinical implications of preserved ratio impaired spirometry: a UK Biobank cohort analysis.Lancet Respir Med. 2022 Feb;10(2):149-157. doi: 10.1016/S2213-2600(21)00369-6. Epub 2021 Nov 2. Lancet Respir Med. 2022. PMID: 34739861
-
Associations Between Physical Activity and Preserved Ratio Impaired Spirometry: A Cross-Sectional NHANES Study.Int J Chron Obstruct Pulmon Dis. 2024 Nov 23;19:2517-2528. doi: 10.2147/COPD.S486447. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 39606713 Free PMC article.
-
Flavonoid intakes, chronic obstructive pulmonary disease, adult asthma, and lung function: a cohort study in the UK Biobank.Am J Clin Nutr. 2024 Nov;120(5):1195-1206. doi: 10.1016/j.ajcnut.2024.08.032. Epub 2024 Aug 31. Am J Clin Nutr. 2024. PMID: 39222688 Free PMC article.
-
Association of systemic inflammatory markers with white matter hyperintensities and microstructural injury: an analysis of UK Biobank data.J Psychiatry Neurosci. 2025 Jan 23;50(1):E45-E56. doi: 10.1503/jpn.240039. Print 2025 Jan-Feb. J Psychiatry Neurosci. 2025. PMID: 39848683 Free PMC article.
-
Association between sex hormones and gout: An analysis of the UK Biobank cohort.Steroids. 2024 Jul;207:109422. doi: 10.1016/j.steroids.2024.109422. Epub 2024 Apr 9. Steroids. 2024. PMID: 38599307
References
-
- Tao H, Mo Y, Liu W, Wang H. A review on gout: Looking back and looking ahead. Int Immunopharmacol. 2023;117: 109977. 10.1016/j.intimp.2023.109977. - PubMed
-
- Dehlin M, Jacobsson L, Roddy E. Global epidemiology of gout: prevalence, incidence, treatment patterns and risk factors. Nat Rev Rheumatol. 2020;16:380–90. 10.1038/s41584-020-0441-1. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
