

Extensive cervical lesion and treatment outcomes in women with HIV/HPV co-infection
- PMID: 39736742
- PMCID: PMC11684313
- DOI: 10.1186/s12981-024-00693-6
Extensive cervical lesion and treatment outcomes in women with HIV/HPV co-infection
Erratum in
-
Correction: Extensive cervical lesion and treatment outcomes in women with HIV/HPV co-infection.AIDS Res Ther. 2025 Apr 7;22(1):46. doi: 10.1186/s12981-025-00736-6. AIDS Res Ther. 2025. PMID: 40197494 Free PMC article. No abstract available.
Abstract
Background: Cervical cancer is a common cancer worldwide, with > 85% of deaths occurring in Lower- and Middle-Income Countries where resources for screening programs are limited. Women living with HIV (WLHIV) are at increased risk. HPV test-and-treat is a screening strategy where women with HPV are offered ablative treatment of the cervix to reduce the risk of invasive cancer. WLHIV tend to have more extensive cervical lesions, necessitating more specialised surgical treatments.
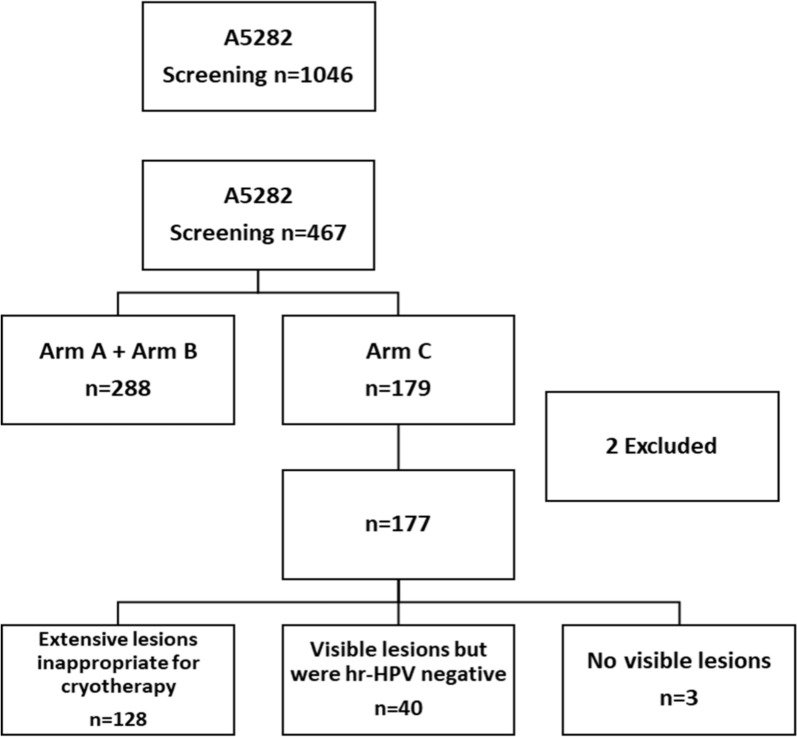
Method: ACTG A5282 was a randomised, open-label, Phase 2 trial conducted in seven countries that compared a cytology-based screening strategy to HPV test-and-treat for cervical cancer prevention in WLHIV. Women with cervical lesions inappropriate for ablative treatment were assigned to Arm C and underwent colposcopy and directed biopsies. Loop electro-excision procedure was performed if high-grade lesions (bHSIL) were present on cervical biopsies. Women were followed 26 weeks later for repeat evaluations. The Clopper-Pearson exact method was used to construct the 95% confidence interval for the proportion of WLHIV with lesions inappropriate for cryotherapy. Logistic regression models were used to assess the factors associated with these lesions.
Results: Of 1046 women screened, 156 (88%) were Black/Non-Hispanic, with a median age of 36 years; 80% were on ART, and 73% had an HIV-1 RNA < 200 copies/mL. On cervical colposcopy, 17% (179/1046, 95% CI 14.9-19.4%) had cervical lesions inappropriate for cervical ablation. Among 428 (44%) women with High-risk HPV (hrHPV) detected, 112 (26%, 95% CI 22.2%, 30.5%) had cervical lesions inappropriate for ablative therapy. hrHPV was found more commonly among women having lesions inappropriate for ablative therapy as compared to lesions appropriate for ablative therapy (70% vs 54%, p < .001). Among 128 women with extensive cervical lesions undergoing colposcopic biopsies, 43 (34%) had bHSIL detected. Among women undergoing LEEP treatment of bHSIL, 24% had bHSIL detected 26 weeks later.
Conclusion: Cervical lesions inappropriate for ablative therapy were common among WLHIV. This has implications for cervical cancer programs as these lesions can only be optimally treated with surgical therapies such as loop electroexcision procedures, and the capacity for this procedure should be increased to maximise cervical cancer prevention outcomes.
Keywords: Cervical cancer; Co-infection; Cytology; HIV care continuum; HPV; Women.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The trial was approved by each site’s institutional review board or ethics committee. Each participant signed informed consent forms prior to being enrolled in the study. This study is registered in ClinicalTrials.gov [NCT01315353]. Consent for publication: All authors shared the final responsibility and consent for submitting for publication. Competing interests: The authors declare no competing interests.
Figures

References
-
- World Health Organization (WHO) International Agency for Reseearch on Cancer (IARC). Estimated age-standardised incidence rates (World) in 2020, Africa, both sexes, all ages (excl. NMSC). https://gco.iarc.who.int/media/globocan/factsheets/populations/903-afric.... Accessed 04 Nov 2022.
