

Impact of Janus kinase inhibitors and methotrexate on interstitial lung disease in rheumatoid arthritis patients
- PMID: 39737175
- PMCID: PMC11683115
- DOI: 10.3389/fimmu.2024.1501146
Impact of Janus kinase inhibitors and methotrexate on interstitial lung disease in rheumatoid arthritis patients
Abstract
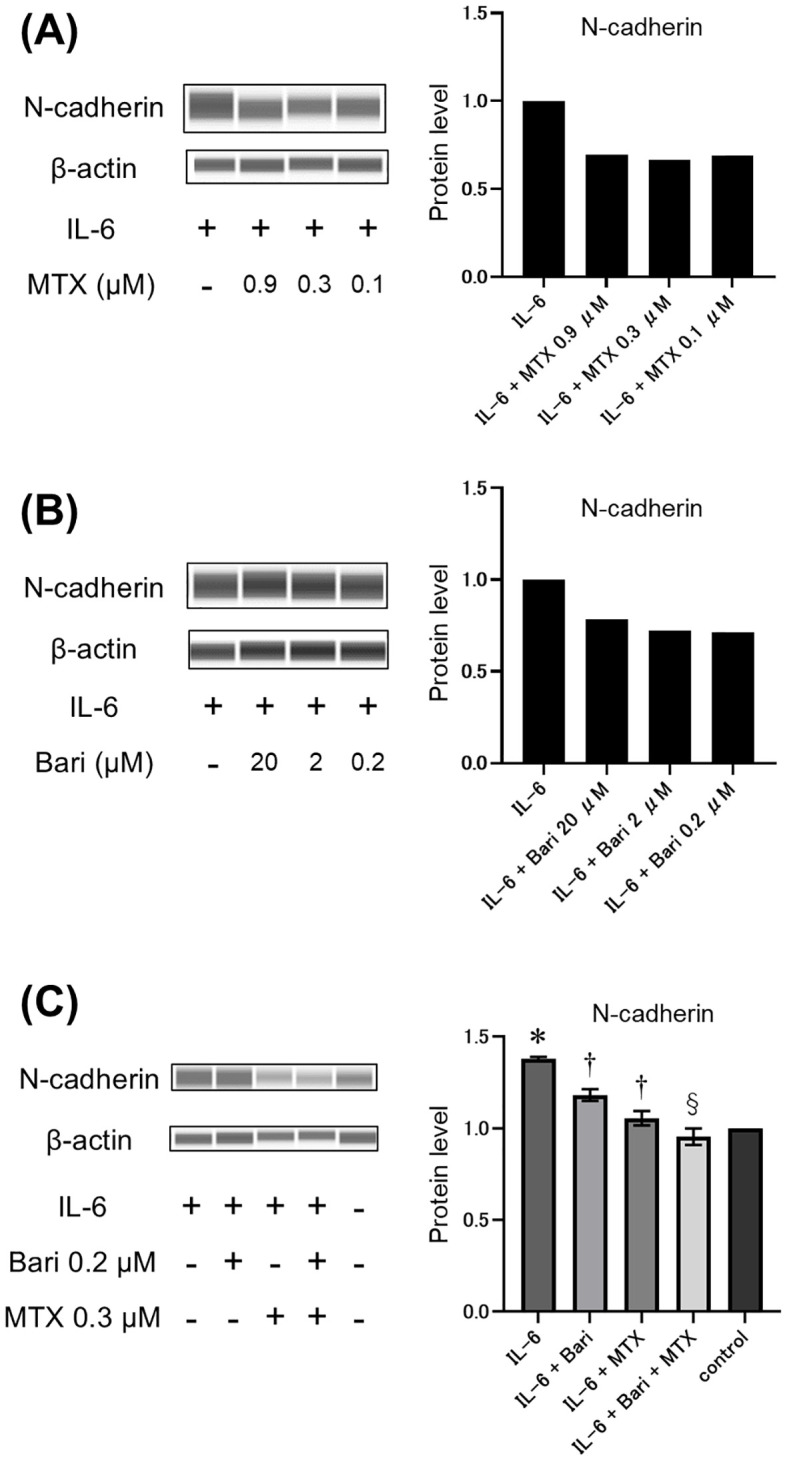
Objectives: Little is known about how various treatments impact the progression of interstitial lung disease (ILD) in rheumatoid arthritis (RA) patients. Here, we compared ILD progression in RA patients treated with Janus kinase inhibitors (JAKi) or biological disease-modifying anti-rheumatic drugs (bDMARDs). In vitro experiments were also performed to evaluate the potential effects of the drugs on epithelial-mesenchymal transition (EMT), a key event in pulmonary fibrosis.
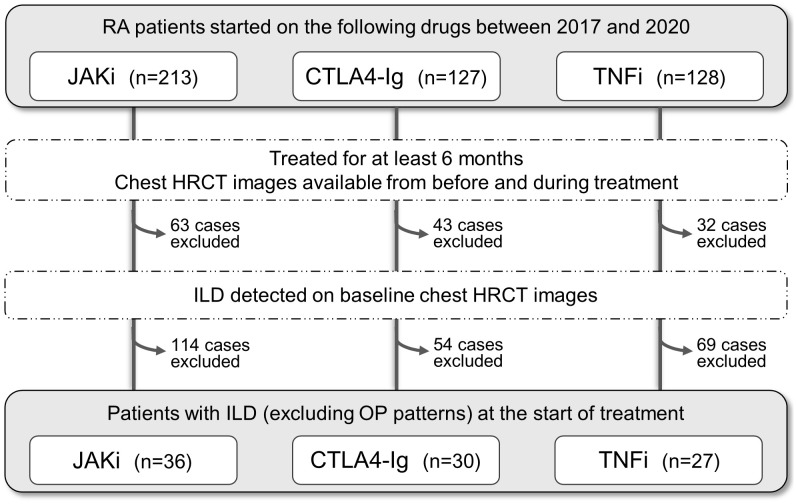
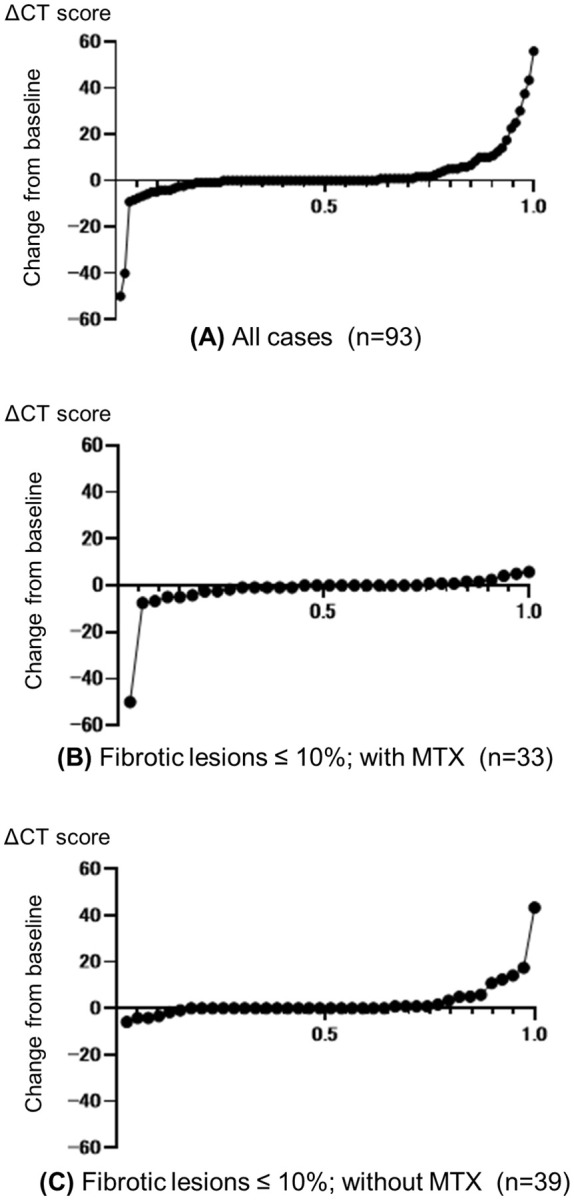
Methods: This retrospective study included 93 RA-ILD patients who initiated treatment with JAKi, tumour necrosis factor inhibitors (TNFi), or abatacept between 2017 and 2020. Worsening ILD was quantified by changes in chest computed tomography (CT) scans between baseline and follow-up (mean 14 months, range 6-51 months). Response to treatment was evaluated using Disease Activity Score-28 with erythrocyte sedimentation rate (DAS28-ESR). Expression of the EMT marker N-cadherin in A549 lung cells was assessed by western blotting.
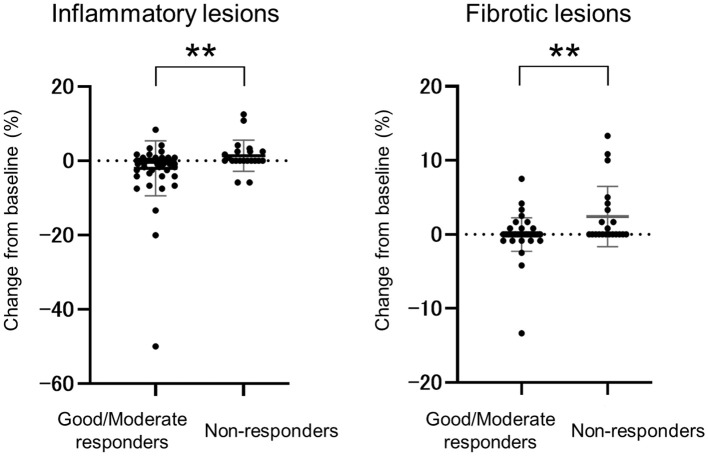
Results and discussion: Worsening ILD was detected in 19.4% (7/36), 16.7% (5/30), and 22.2% (6/27) of patients treated with JAKi, abatacept, and TNFi, respectively. Multivariate analysis identified female gender (P=0.043) and >10% fibrotic lesions (P=0.015) as significant predictors of worsening ILD. DAS28-ESR-based non-responder status was also significantly associated with worsening ILD (P=0.0085). In vitro, combination treatment with methotrexate and baricitinib significantly impeded EMT progression. Worsening ILD was associated with more extensive fibrotic lesions at baseline and female gender in RA patients treated with JAKi or bDMARDs. JAKi and methotrexate co-treatment may prove beneficial in modifying key events underlying the pathogenesis of RA-ILD.
Keywords: JAK inhibitors; RA-ILD; epithelial-mesenchymal transition; interstitial lung disease; methotrexate; rheumatoid arthritis.
Copyright © 2024 Kurushima, Koga, Umeda, Iwamoto, Miyashita, Tokito, Okuno, Yura, Ishimoto, Kido, Sakamoto, Ueki, Mukae and Kawakami.
Conflict of interest statement
TK and AK received honoraria for speaking engagements from Eli Lilly, Japan. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential conflict of interest.
Figures
Similar articles
-
A retrospective study of the efficacy of JAK inhibitors or abatacept on rheumatoid arthritis-interstitial lung disease.Inflammopharmacology. 2022 Jun;30(3):705-712. doi: 10.1007/s10787-022-00936-w. Epub 2022 Apr 24. Inflammopharmacology. 2022. PMID: 35462572 Free PMC article.
-
Effect of abatacept versus conventional synthetic disease modifying anti-rheumatic drugs on rheumatoid arthritis-associated interstitial lung disease.Korean J Intern Med. 2024 Sep;39(5):855-864. doi: 10.3904/kjim.2023.207. Epub 2024 Aug 30. Korean J Intern Med. 2024. PMID: 39252490 Free PMC article.
-
Radiological evaluation of interstitial lung disease in patients with rheumatoid arthritis treated with abatacept or JAK inhibitors for 1 year.Respir Investig. 2023 May;61(3):359-363. doi: 10.1016/j.resinv.2023.02.007. Epub 2023 Apr 7. Respir Investig. 2023. PMID: 37031622
-
Janus kinase inhibitors in rheumatoid arthritis-associated interstitial lung disease: A systematic review and meta-analysis.Autoimmun Rev. 2024 Oct;23(10):103636. doi: 10.1016/j.autrev.2024.103636. Epub 2024 Sep 11. Autoimmun Rev. 2024. PMID: 39270812
-
Rheumatoid arthritis-associated interstitial lung disease: an overview of epidemiology, pathogenesis and management.Clin Rheumatol. 2021 Apr;40(4):1211-1220. doi: 10.1007/s10067-020-05320-z. Epub 2020 Aug 13. Clin Rheumatol. 2021. PMID: 32794076 Review.
Cited by
-
Role of Interleukin-6 in Rheumatoid Arthritis-Associated Interstitial Lung Disease: Focus on the JAK/STAT Pathway and Macrophage Polarization.J Inflamm Res. 2025 Aug 13;18:10953-10967. doi: 10.2147/JIR.S530754. eCollection 2025. J Inflamm Res. 2025. PMID: 40827265 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous