

Metformin improves Mycobacterium avium infection by strengthening macrophage antimicrobial functions
- PMID: 39737195
- PMCID: PMC11682992
- DOI: 10.3389/fimmu.2024.1463224
Metformin improves Mycobacterium avium infection by strengthening macrophage antimicrobial functions
Abstract
Introduction: The incidence and prevalence of infections with non-tuberculous mycobacteria such as Mycobacterium avium (Mav) are increasing. Prolonged drug regimens, inherent antibiotic resistance, and low cure rates underscore the need for improved treatment, which may be achieved by combining standard chemotherapy with drugs targeting the host immune system. Here, we examined if the diabetes type 2 drug metformin could improve Mav-infection.
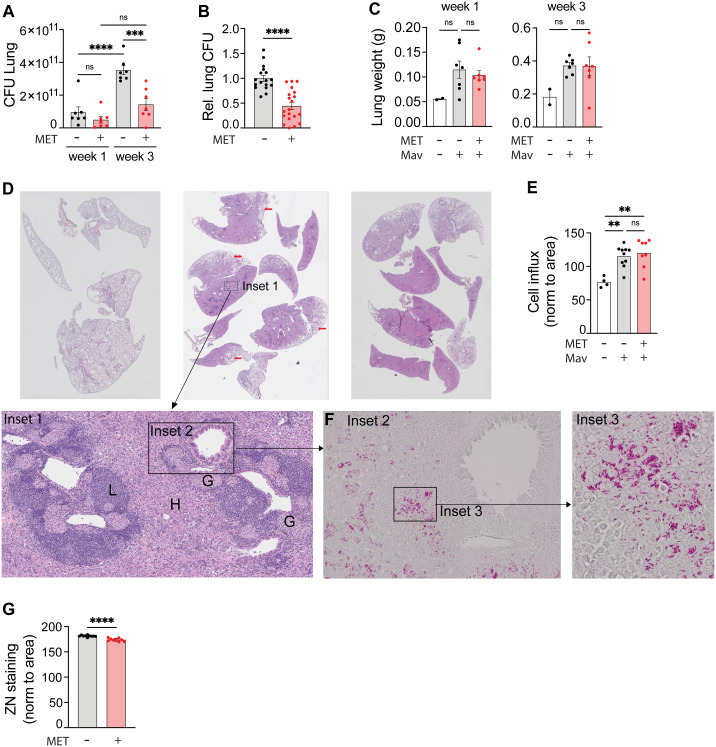
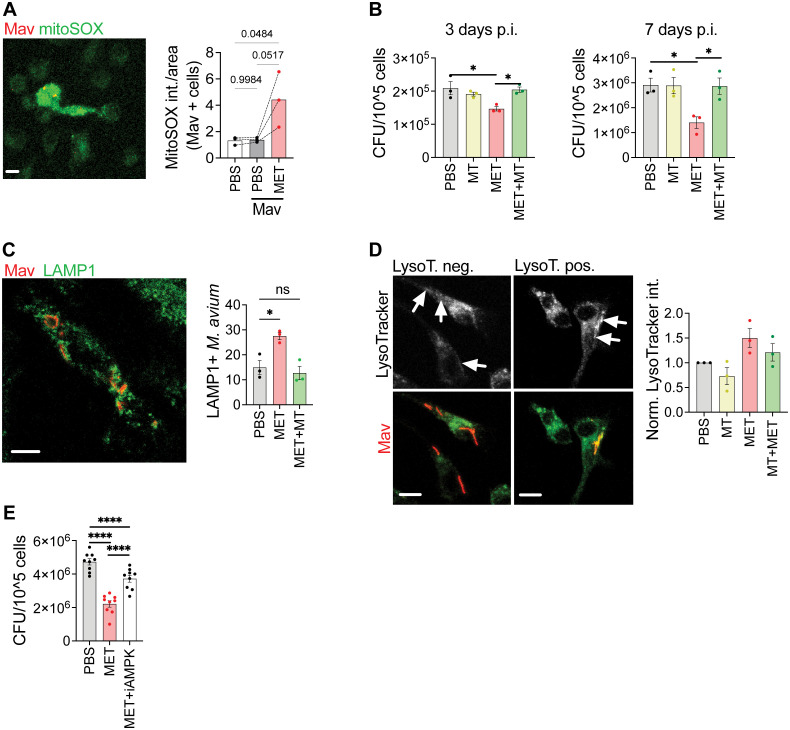
Methods: Metformin was administered to C57BL/6 mice infected intranasally with Mav and C57BL/6 mice were infected intranasally with Mav and treated with metformin over 3 weeks. Organ bacterial loads and lung pathology, inflammatory cytokines and immune cell profiles were assessed. For mechanistic insight, macrophages infected with Mav were treated with metformin alone or in combination with inhibitors for mitochondrial ROS or AMPK and assessed for bacterial burden and phagosome maturation.
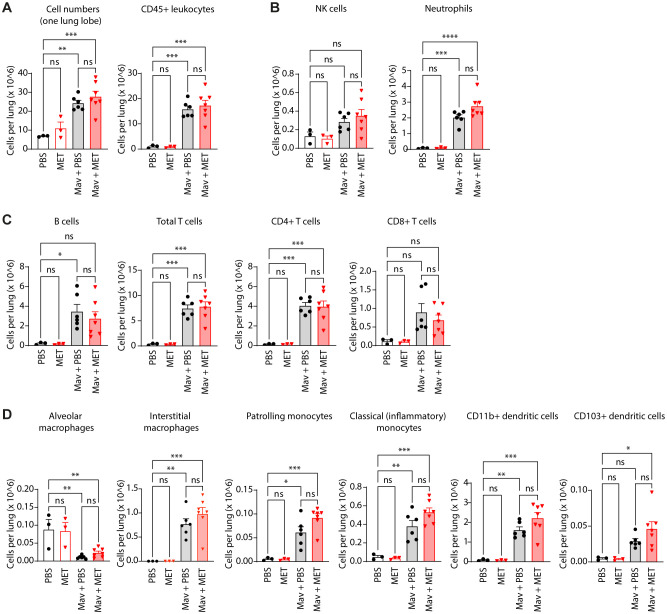
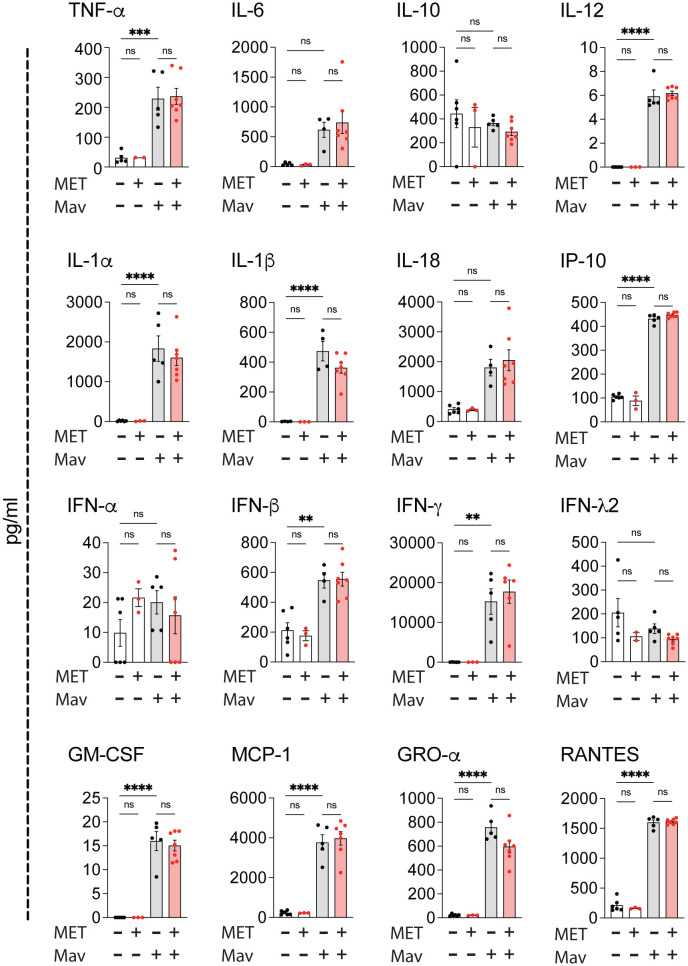
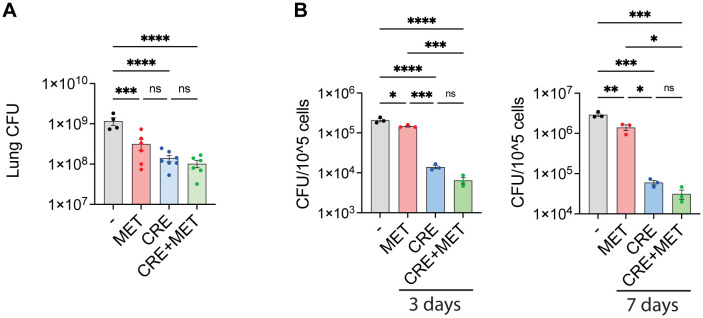
Results and discussion: Three weeks of metformin treatment significantly reduced the lung mycobacterial burden in mice infected with Mav without major changes in the overall lung pathology or immune cell composition. Metformin treatment had no significant impact on tissue inflammation except for a tendency of increased lung IFNγ and infiltration of Mav-specific IFNγ-secreting T cells. Metformin did, however, boost the antimicrobial capacity of infected macrophages directly by modulating metabolism/activating AMPK, increasing mitochondrial ROS and phagosome maturation, and indirectly by bolstering type I immunity. Taken together, our data show that metformin improved the control of Mav-infection in mice, mainly by strengthening antimicrobial defenses in macrophages, and suggest that metformin has potential as an adjunct treatment of Mav infections.
Keywords: Metformin; Mycobacterium avium; host-directed therapy; macrophage; mouse; non-tuberculous.
Copyright © 2024 Mediaas, Haug, Louet, Wahl, Gidon and Flo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
Similar articles
-
Phenothiazines boost host control of Mycobacterium avium infection in primary human macrophages.Biomed Pharmacother. 2025 Apr;185:117941. doi: 10.1016/j.biopha.2025.117941. Epub 2025 Feb 27. Biomed Pharmacother. 2025. PMID: 40020517
-
Apoptosis inhibitor of macrophage suppress immune responses via IL-10 production and delay bacterial clearance in Mycobacterium avium infection.Front Cell Infect Microbiol. 2025 May 5;15:1578082. doi: 10.3389/fcimb.2025.1578082. eCollection 2025. Front Cell Infect Microbiol. 2025. PMID: 40391046 Free PMC article.
-
Development of Human Cell-Based In Vitro Infection Models to Determine the Intracellular Survival of Mycobacterium avium.Front Cell Infect Microbiol. 2022 Jun 24;12:872361. doi: 10.3389/fcimb.2022.872361. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 35811670 Free PMC article.
-
Identification of virulence determinants of Mycobacterium avium that impact on the ability to resist host killing mechanisms.J Med Microbiol. 2010 Jan;59(Pt 1):8-16. doi: 10.1099/jmm.0.012864-0. J Med Microbiol. 2010. PMID: 19745033 Free PMC article.
-
Modulating macrophage function to reinforce host innate resistance against Mycobacterium avium complex infection.Front Immunol. 2022 Nov 24;13:931876. doi: 10.3389/fimmu.2022.931876. eCollection 2022. Front Immunol. 2022. PMID: 36505429 Free PMC article. Review.
Cited by
-
Metformin carbon dots-based osteogenic and protein delivery system to promote bone regeneration in periodontitis.Bioact Mater. 2025 Jul 25;53:459-479. doi: 10.1016/j.bioactmat.2025.07.001. eCollection 2025 Nov. Bioact Mater. 2025. PMID: 40747455 Free PMC article.
References
-
- van Ingen J, Obradovic M, Hassan M, Lesher B, Hart E, Chatterjee A, et al. . Nontuberculous mycobacterial lung disease caused by Mycobacterium avium complex - disease burden, unmet needs, and advances in treatment developments. Expert Rev Respir Med. (2021) . 15:1387–401. doi: 10.1080/17476348.2021.1987891 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources