

Durvalumab and tremelimumab in patients with advanced rare cancer: a multi-centre, non-blinded, open-label phase II basket trial
- PMID: 39737219
- PMCID: PMC11683278
- DOI: 10.1016/j.eclinm.2024.102991
Durvalumab and tremelimumab in patients with advanced rare cancer: a multi-centre, non-blinded, open-label phase II basket trial
Abstract
Background: Dual inhibition of cytotoxic T-lymphocyte associated protein 4 (CTLA-4) and programmed death ligand 1 (PD-L1) has been shown to be an effective treatment strategy in many cancers. We sought to determine the objective response rate of combination durvalumab (D) plus tremelimumab (TM) in parallel cohorts of patients with carefully selected rare cancer types in which these agents had not previously been evaluated in phase II trials and for which there was clinical or biological rationale for dual immune checkpoint inhibitor therapy to be active.
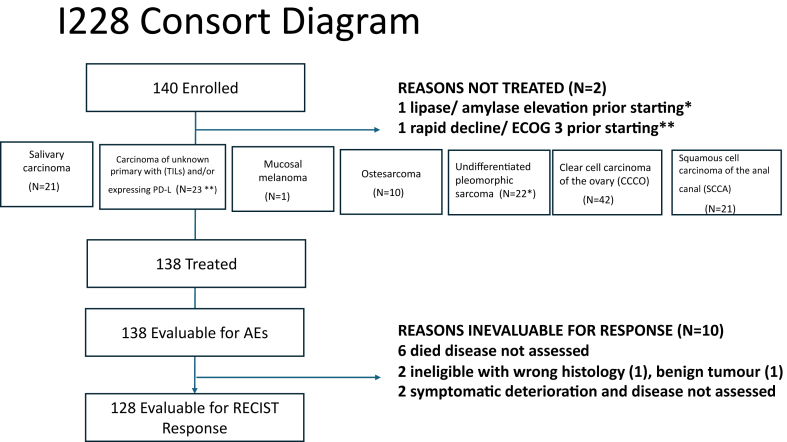
Methods: We designed a multi-centre, non-blinded, open-label phase II basket trial with each of the following 8 rare cancers considered a separate phase II trial: salivary carcinoma, carcinoma of unknown primary (CUP) with tumour infiltrating lymphocytes and/or expressing PD-L1, mucosal melanoma, acral melanoma, osteosarcoma, undifferentiated pleomorphic sarcoma, clear cell carcinoma of the ovary (CCCO) or squamous cell carcinoma of the anal canal (SCCA). The primary objective was to evaluate the response rate of the combination of D and TM, and the secondary objectives were to evaluate the tolerability and safety of D and TM combination. Eligible patients had advanced, metastatic or recurrent, or unresectable cancer with no known life-prolonging treatment option, age ≥16 years, ECOG performance status 0 or 1. Patients received D (1500 mg IV) + TM (75 mg IV) on Day 1 q4 weeks for 4 cycles followed by D q4 weeks until disease progression. This trial is registered with ClinicalTrials.gov, NCT02879162.
Findings: From December 14th, 2016, to August 14, 2019, 140 patients enrolled into seven cohorts. The rare melanoma cohorts were closed due to lack of accrual. Of the 140 patients enrolled, 138 were eligible, 138 were evaluable for toxicity and 128 (91%) were evaluable for response. Durable responses were noted in all cohorts except for osteosarcoma. The overall response rate for eligible patients was 16% (95% CI: 10-23%). The response rates in each cancer cohort were undifferentiated pleomorphic sarcoma 15% (n = 3/20; 95% CI 3-38%), salivary carcinoma 20% (n = 4/20; 95% CI: 6-44%), CUP 17% (n = 3/18; 95% CI 4-41%), SCCA 10% (n = 2/20; 95% CI 12-32%) and CCCO 21% (n = 8/39; 95% CI 9-37%). Grade 3/4 adverse events were rare, where 4 patients experienced grade 4 related events and39 patients experienced grade 3 events.
Interpretation: Durvalumab + tremelimumab treatment resulted in meaningful responses in salivary carcinoma and CCCO and deserves further exploration in front-line studies.
Funding: AstraZeneca and Canadian Cancer Society.
Keywords: Checkpoint inhibitors; Ovarian carcinoma; Rare cancers.
© 2024 The Author(s).
Conflict of interest statement
AT–Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: GSK, AZ, Eisai, Merck/Support for attending meetings and/or travel: GSK/Participation on a Data Safety Monitoring Board or Advisory Board: GSK, Eisai, Merck. RJ–Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: Pfizer/Participation on a Data Safety Monitoring Board or Advisory Board: BMS, Medison. HH–Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: Novocure Canada/Participation on a Data Safety Monitoring Board or Advisory Board: Novocure Canada. EW–Grants or contracts: Merck, Roche/Genetech/Consulting fees: Merck, Roche, EMD Serono. QC–Grants or contracts: AZ/Consulting fees: Abbvie, Amgen, AnHeart, Astellas, AZ, Boehringer Ingelheim, Bristol Meyer Squibb, Daichii Sankyo, Eli Lilly, GSK, Janssen, Merck, Novartis, Ocellaris, Pfizer, Roche, Takeda/Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: Abbvie, Amgen, AnHeart, Astellas, Astra Zeneca, Boehringer Ingelheim, Bristol Meyer Squibb, Diachii Sankyo, Eli Lilly, GSK, Janssen, Merck, Novartis, Ocellaris, Pfizer, Roche, Takeda/Participation on a Data Safety Monitoring Board or Advisory Board: Merck, Serano/Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid: Lung Cancer Canada. CK–Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: Astellas, Bayer, BMS, Merck, Pfizer, Janssen, Eisai, Seagen, Ipsen, Abbvie, AstraZeneca/Support for attending meetings and/or travel: Ipsen, Novartis, Janssen, AstraZeneca/Participation on a Data Safety Monitoring Board or Advisory Board: Ipsen, BMS, Eisai, Novartis, Astellas, Bayer, AstraZeneca, Merck, Pfizer, BioTech, Seagen, Abbvie, TA–Consulting fees: BMS, Roche, AZ, Merck, Bayer/Support for attending meetings and/or Travel: Spring Works Therapeutics. TN–All support for the present manuscript (e.g., funding, provision of study materials, medical writing, article processing charges, etc.): CCS. DP–Grants or contracts: Exactis/Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: GSK, AZ/Participation on a Data Safety Monitoring Board or Advisory Board: Exactis JH–Consulting fees: BMS, AZ, Novartis, Eli-Lilly, Seattle Genetics, Gilead/Participation in data safety monitoring board or advisory board: BMS. MK–All support for the present manuscript (e.g., funding, provision of study materials, medical writing, article processing charges, etc.): AZ/Grants or contracts: Eisai, Exelixis, Novartis, Eli Lilly/Consulting fees: Bayer/Participation on a Data Safety Monitoring Board or Advisory Board: Bayer, Ipsen. SH–Consulting fees: BMS, Merck. JD–Grants or contacts: AZ. All other authors have no conflicts to declare.
Figures
References
-
- Fife B.T., Bluestone J.A. Control of peripheral T-cell tolerance and autoimmunity via the CTLA-4 and PD-1 pathways. Immunol Rev. 2008;224:166–182. - PubMed
-
- Brahmer J.R. PD-1-targeted immunotherapy: recent clinical findings. Clin Adv Hematol Oncol. 2012;10(10):674–675. - PubMed
-
- Eggermont A.M.M., Blank C.U., Mandala M., et al. Adjuvant pembrolizumab versus placebo in resected stage III melanoma. N Engl J Med. 2018;378(19):1789–1801. - PubMed
-
- Weber J., Mandala M., Del Vecchio M., et al. Adjuvant nivolumab versus ipilimumab in resected stage III or IV melanoma. N Engl J Med. 2017;377(19):1824–1835. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
