

Standardized protocol for labor induction: a type I hybrid effectiveness-implementation trial
- PMID: 39737251
- PMCID: PMC11683308
- DOI: 10.1016/j.lana.2024.100956
Standardized protocol for labor induction: a type I hybrid effectiveness-implementation trial
Abstract
Background: Cesarean delivery remains the most common obstetrical procedure with more than 250,000 patients in the US undergoing cesarean following labor induction annually. Here, we evaluated the impact of prospectively implementing a standardized labor induction protocol on cesarean delivery rates.
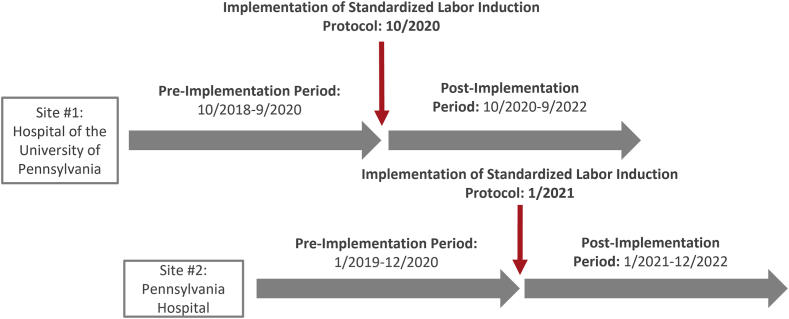
Methods: This multi-site type I hybrid effectiveness-implementation study compared 2 years before (PRE) and 2 years after (POST) implementation of a standardized labor induction protocol at two hospitals within the University of Pennsylvania Health System (2018-2022). The protocol included multiple components and recommended active management of labor induction, including frequent cervical examinations, amniotomy if cervical exam ≥4 cm, and interventions for labor dystocia. The primary effectiveness outcome was cesarean delivery. Secondary effectiveness outcomes included labor length, chorioamnionitis, and maternal and neonatal morbidity. The primary implementation outcome was fidelity, defined as adherence to ≥75% of the protocol components among 8 individual components that could be evaluated discretely. All data was collected via individual chart review.
Findings: 8509 patients were included (PRE: n = 4214, POST: n = 4295). Our population was of median age of 31 years interquartile range (IQR) [26-35], and 44.6% identified as Black, 40.1% as white, 6.9% as Asian, and 8.4% as other or unknown; 7.4% of the population identified as Latinx. There was no significant difference in cesarean delivery rate between the two time periods overall (PRE: 21.6% vs. POST: 21.8%, p = 0.85; adjusted relative risk (aRR) 0.99 95% confidence interval (CI) [0.90-1.09]). There were no significant differences in labor length, chorioamnionitis, or composite neonatal morbidity. Maternal morbidity decreased PRE to POST (PRE: 9.3% vs. POST: 6.5%, p < 0.001; aRR 0.67 95% CI [0.58-0.79]). POST-implementation, inductions with fidelity to ≥75% of protocol components increased (PRE: 52.4% vs. POST: 59.6%, p < 0.001), evidenced by more frequent cervical examinations, earlier dilation at amniotomy, and increased labor dystocia management.
Interpretation: Despite increasing standardized induction management, no significant difference in cesarean delivery was found.
Funding: NICHD K23HD102523.
Keywords: Cesarean delivery; Fidelity; Implementation science; Labor induction; Maternal morbidity; Protocols; Standardization.
© 2024 The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Similar articles
-
A standardized labor induction protocol: impact on racial disparities in obstetrical outcomes.Am J Obstet Gynecol MFM. 2020 Aug;2(3):100148. doi: 10.1016/j.ajogmf.2020.100148. Epub 2020 Jun 5. Am J Obstet Gynecol MFM. 2020. PMID: 33345879 Clinical Trial.
-
Impacts of embracing 39-week elective induction across an entire labor and delivery unit.AJOG Glob Rep. 2023 Jan 29;3(2):100168. doi: 10.1016/j.xagr.2023.100168. eCollection 2023 May. AJOG Glob Rep. 2023. PMID: 36941864 Free PMC article.
-
Identifying the effective components of a standardized labor induction protocol: secondary analysis of a randomized, controlled trial.J Matern Fetal Neonatal Med. 2022 Dec;35(25):6185-6191. doi: 10.1080/14767058.2021.1909561. Epub 2021 Apr 13. J Matern Fetal Neonatal Med. 2022. PMID: 33847224 Free PMC article.
-
Early vs. delayed amniotomy in individuals undergoing pre-induction cervical ripening with transcervical Foley balloon: a meta-analysis.Am J Obstet Gynecol MFM. 2024 Aug;6(8):101408. doi: 10.1016/j.ajogmf.2024.101408. Epub 2024 Jun 17. Am J Obstet Gynecol MFM. 2024. PMID: 38897352
-
Effects of induction of labor prior to post-term in low-risk pregnancies: a systematic review.JBI Database System Rev Implement Rep. 2019 Feb;17(2):170-208. doi: 10.11124/JBISRIR-2017-003587. JBI Database System Rev Implement Rep. 2019. PMID: 30299344 Free PMC article.
Cited by
-
Audit and feedback is an effective implementation strategy to increase fidelity to a multi-component labor induction protocol designed to reduce obstetric inequities.Implement Sci Commun. 2025 Jan 3;6(1):2. doi: 10.1186/s43058-024-00681-x. Implement Sci Commun. 2025. PMID: 39754232 Free PMC article.
References
-
- American College of Obstetricians and Gynecologists (College) Society for Maternal-Fetal Medicine. Caughey A.B., Cahill A.G., Guise J.M., Rouse D.J. Safe prevention of the primary cesarean delivery. Am J Obstet Gynecol. 2014;210(3):179–193. - PubMed
-
- Koroukian S.M., Trisel B., Rimm A.A. Estimating the proportion of unnecessary Cesarean sections in Ohio using birth certificate data. J Clin Epidemiol. 1998;51(12):1327–1334. - PubMed
-
- Kabir A.A., Steinmann W.C., Myers L., et al. Unnecessary cesarean delivery in Louisiana: an analysis of birth certificate data. Am J Obstet Gynecol. 2004;190(1):10–19. - PubMed
-
- Hamm R.F., Moniz M.H., Wahid I., Breman R.B., Callaghan-Koru J.A., Implementation Science for Maternal Health National Working G Implementation research priorities for addressing the maternal health crisis in the USA: results from a modified Delphi study among researchers. Implement Sci Commun. 2023;4(1):83. - PMC - PubMed
LinkOut - more resources
Full Text Sources
