

Performance of Risk-Stratification Scores for Patients With Pulmonary Arterial Hypertension in a Multi-Ethnic Asian Population
- PMID: 39737392
- PMCID: PMC11682694
- DOI: 10.1002/pul2.70032
Performance of Risk-Stratification Scores for Patients With Pulmonary Arterial Hypertension in a Multi-Ethnic Asian Population
Abstract
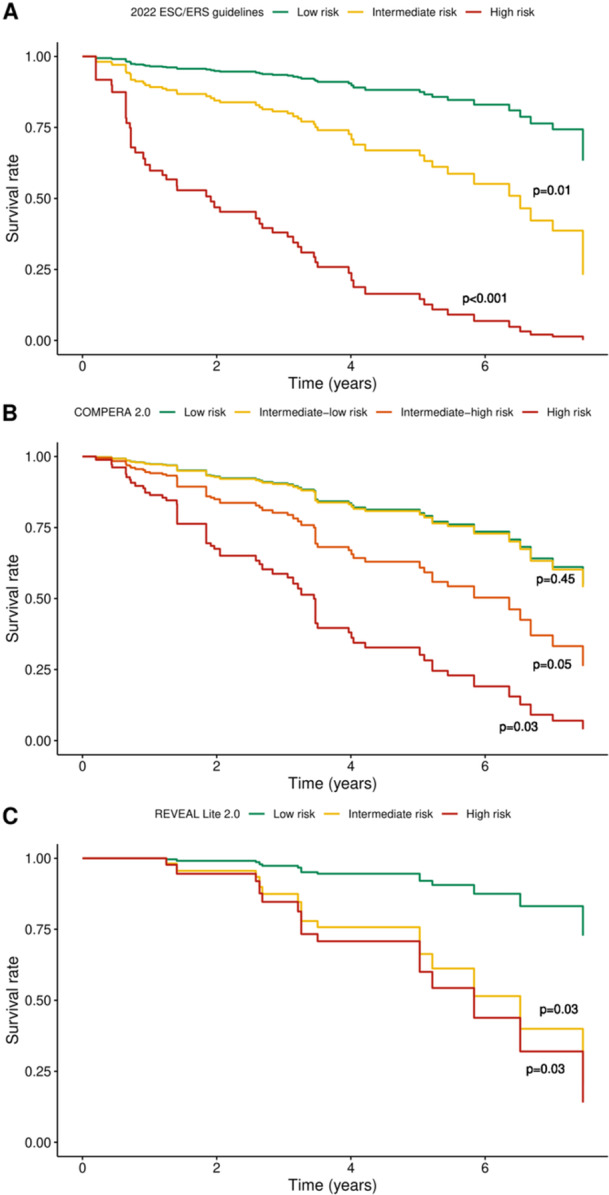
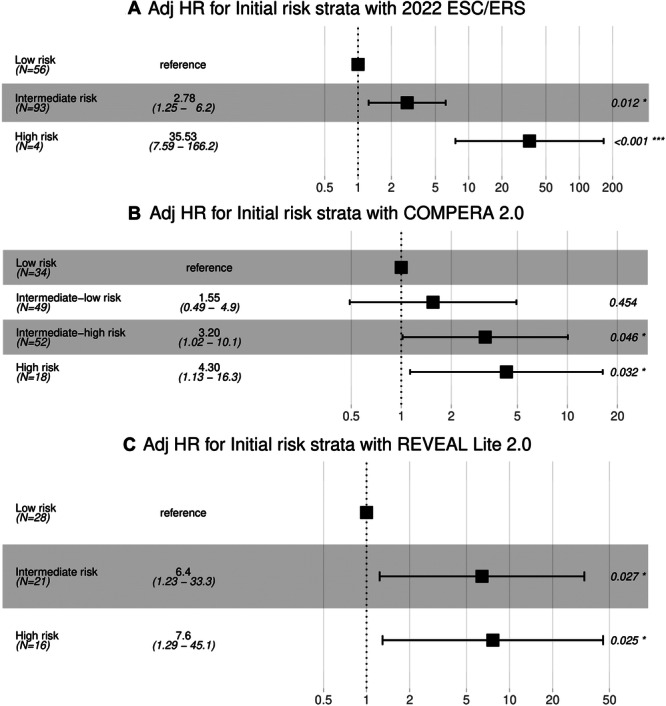
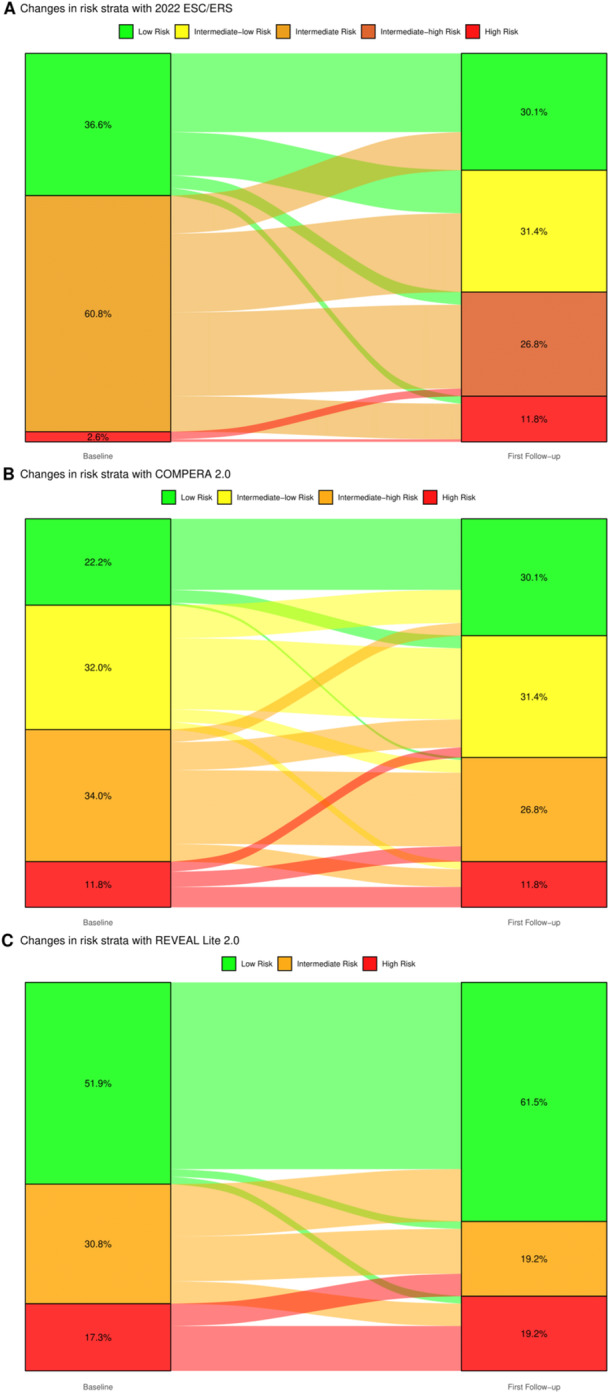
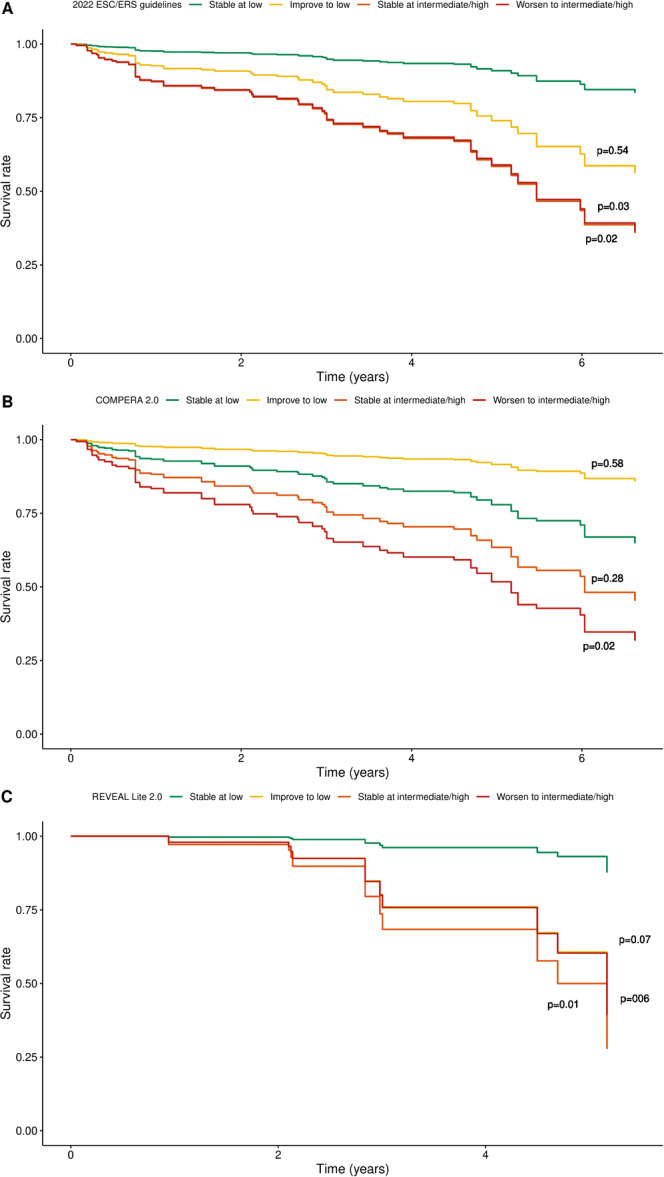
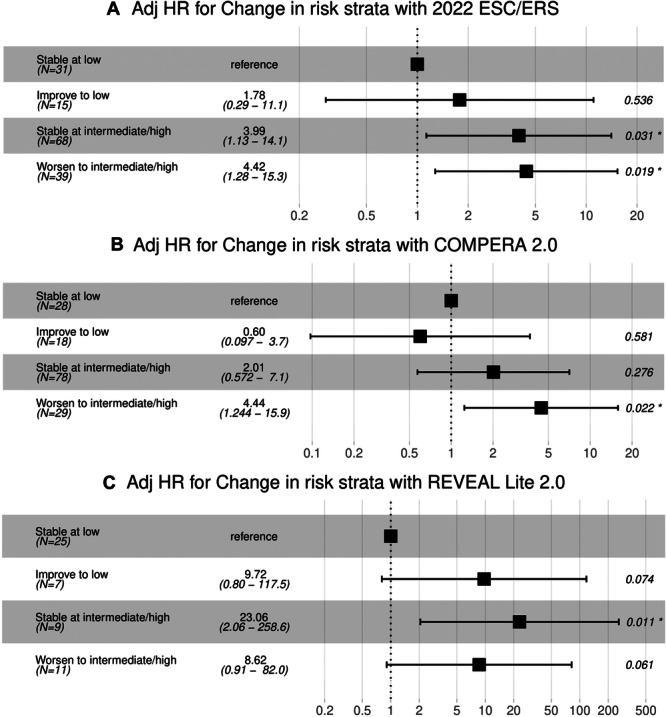
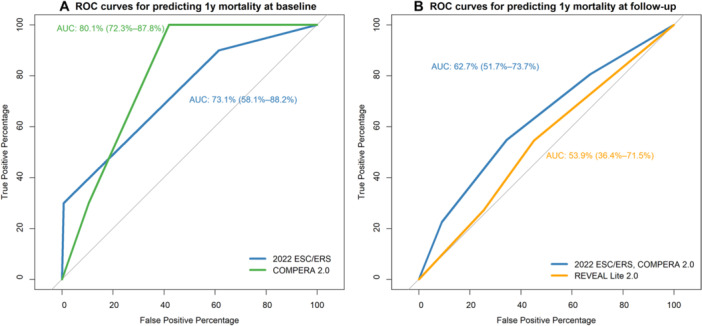
Guidelines recommend risk stratification of pulmonary arterial hypertension (PAH) patients to guide management. There are currently several risk stratification scores available, which have largely been validated in various pulmonary hypertension registries in the West but not in Asia. We aim to study the performance of these different risk scores in PAH patients from a multi-ethnic Asian population. A retrospective review of all PAH patients from Jan 2014 to Jun 2021 from a tertiary cardiac center was performed. Mortality outcomes were obtained from national registries. Using the 2022 ESC/ERS, REVEAL Lite 2.0 and COMPERA 2.0 risk scores, patients were classified into different risk strata at baseline and at follow-up and changes in any risk strata recorded. The prognosis of patients based on these factors was compared. A total of 153 patients (mean age: 57 ± 17 years; 117 women; 94 Chinese, 33 Malay, 19 Indian) were included. All three scores showed significant difference in mortality outcomes between the different risk strata both at baseline and at follow-up (p < 0.05), with the highest risk group showing the highest mortality. Patients who worsened to or remained at intermediate/high-risk generally had a worse prognosis than those who remained stable at or improved to low-risk strata. The 2022 ESC/ERS and COMPERA 2.0 risk scores had C-statistics of 0.73 (0.58-0.88) and 0.80 (0.72-0.88), respectively, for predicting 1-year mortality. Serial risk stratification is a useful tool in prognosticating Asian PAH patients and may play an important role in guiding therapeutic management.
Keywords: primary pulmonary hypertension; pulmonary arterial hypertension; pulmonary circulation and pulmonary hypertension; risk stratification.
© 2024 The Author(s). Pulmonary Circulation published by Wiley Periodicals LLC on behalf of the Pulmonary Vascular Research Institute.
Conflict of interest statement
JY received speaker's honorarium from Abbott, Biosensors, Biotronik, Boston Scientific, Edwards, GE healthcare, J&J, Kaneka, Medtronic and Terumo. AL received consultancy fees and is on the advisory boards of Janssen and Boehringer‐Ingelheim, and is on the steering committee and received research grants from Boehringer‐Ingelheim. All other authors declare no conflicts of interest.
Figures
References
-
- Benza R. L., Miller D. P., Barst R. J., Badesch D. B., Frost A. E., and McGoon M. D., “An Evaluation of Long‐Term Survival From Time of Diagnosis in Pulmonary Arterial Hypertension From the REVEAL Registry,” Chest 142 (2012): 448–456. - PubMed
-
- Galiè N., Brundage B. H., Ghofrani H. A., et al., “Tadalafil Therapy for Pulmonary Arterial Hypertension,” Circulation 119 (2009): 2894–2903. - PubMed
-
- Galiè N., Ghofrani H. A., Torbicki A., et al., “Sildenafil Citrate Therapy for Pulmonary Arterial Hypertension,” New England Journal of Medicine 353 (2005): 2148–2157. - PubMed
-
- Sitbon O., Sattler C., Bertoletti L., et al., “Initial Dual Oral Combination Therapy in Pulmonary Arterial Hypertension,” European Respiratory Journal 47 (2016): 1727–1736. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
