

Predictive value of trendelenburg position and carotid ultrasound for fluid responsiveness in patients on VV-ECMO with acute respiratory distress syndrome in the prone position
- PMID: 39738306
- PMCID: PMC11685402
- DOI: 10.1038/s41598-024-83038-7
Predictive value of trendelenburg position and carotid ultrasound for fluid responsiveness in patients on VV-ECMO with acute respiratory distress syndrome in the prone position
Abstract
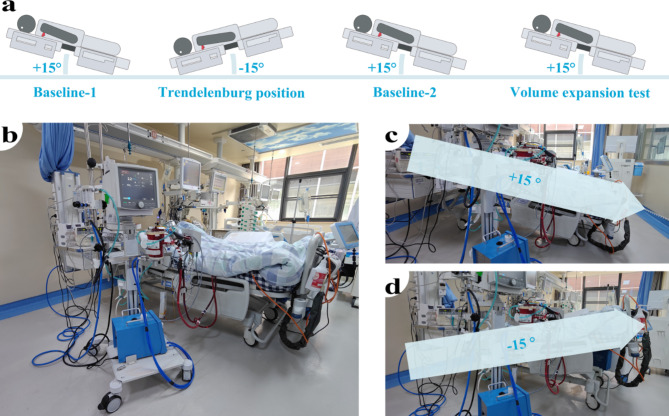
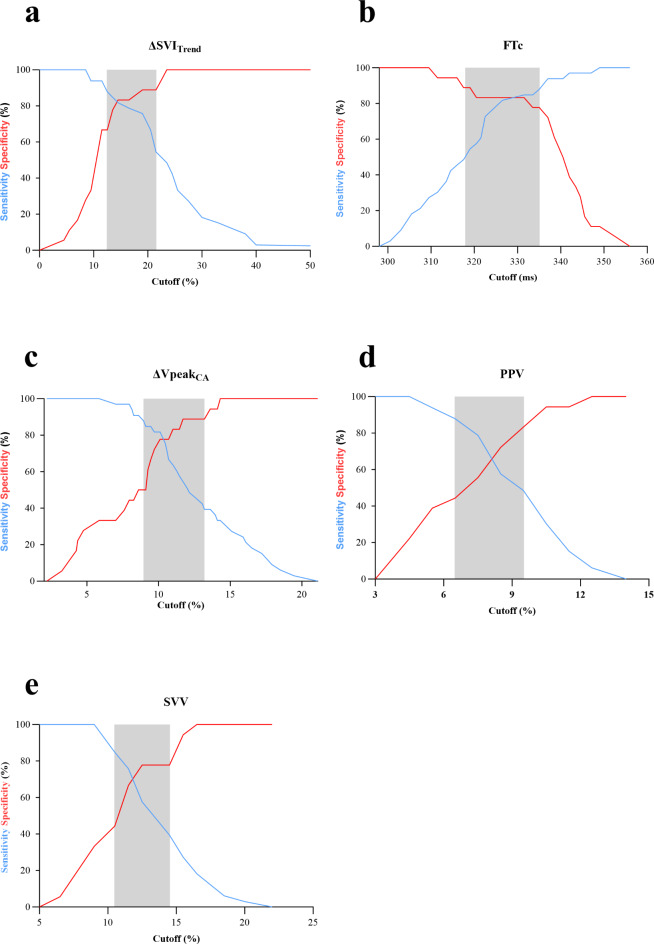
Fluid administration is widely used to treat hypotension in patients undergoing veno-venous extracorporeal membrane oxygenation (VV-ECMO). However, excessive fluid administration may lead to fluid overload can aggravate acute respiratory distress syndrome (ARDS) and increase patient mortality, predicting fluid responsiveness is of great significance for VV-ECMO patients. This prospective single-center study was conducted in a medical intensive care unit (ICU) and finally included 51 VV-ECMO patients with ARDS in the prone position (PP). Stroke volume index variation (ΔSVI), pulse pressure variation (PPV), stroke volume variation (SVV), baseline carotid corrected flow time (FTcBaseline), and respirophasic variation in carotid artery blood flow peak velocity (ΔVpeakCA) were taken before and after the Trendelenburg position or volume expansion. Fluid responsiveness was defined as a 15% or more increase in stroke volume index as assessed by transthoracic echocardiography after the volume expansion (VE). In our study, 33 patients (64.7%) were identified as fluid responders. Stroke volume index variation induced by the Trendelenburg position (ΔSVITrend), FTcBaseline, and ΔVpeakCA demonstrated superior predictive performance of fluid responsiveness. ΔSVITrend had an AUC of 0.89 (95% CI, 0.80-0.98) with an optimal threshold of 14.5% (95% CI, 12.5-21.5%), with the sensitivity and specificity were 82% (95% CI, 66-91%) and 83% (95% CI, 61-94%). FTcBaseline had an AUC of 0.87 (95% CI, 0.76-0.98) with an optimal threshold of 332ms (95% CI, 318-335ms), the sensitivity and specificity were 85% (95% CI, 69-93%) and 83% (95% CI, 61-94%), respectively. ΔVpeakCA showed an AUC of 0.83 (95% CI, 72-95), with a 10% optimal threshold (95% CI, 9-13%), sensitivity was 82% (95% CI, 66-91%) and specificity 78% (95% CI, 55-91%). ΔSVITrend, FTcBaseline and ΔVpeakCA could effectively predict fluid responsiveness in VV-ECMO patients with ARDS in the PP. Compared to ΔSVITrend and ΔVpeakCA, FTcBaseline is easier and more direct to acquire, and it does not require Trendelenburg position or VE, making it a more accessible and efficient option for assessing fluid responsiveness.
Keywords: Carotid ultrasound; Fluid responsiveness; Trendelenburg position; VV-ECMO.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics approval and consent to participate: This prospective, single-center study was conducted in the ICU between May 2022 and February 2024. It was approved by the Institutional Review Board of Quzhou People’s Hospital (Quzhou, China: Number B 2022-083) and performed in accordance with the Declaration of Helsinki. All research was performed in accordance with relevant guidelines/regulations. Informed consent was obtained from all participants and/or their legal guardians. Consent for publication: Not applicable.
Figures




Similar articles
-
Change in cardiac output during Trendelenburg maneuver is a reliable predictor of fluid responsiveness in patients with acute respiratory distress syndrome in the prone position under protective ventilation.Crit Care. 2017 Dec 5;21(1):295. doi: 10.1186/s13054-017-1881-0. Crit Care. 2017. PMID: 29208025 Free PMC article. Clinical Trial.
-
Passive leg raising can predict fluid responsiveness in patients placed on venovenous extracorporeal membrane oxygenation.Crit Care. 2011;15(5):R216. doi: 10.1186/cc10451. Epub 2011 Sep 18. Crit Care. 2011. PMID: 21923944 Free PMC article.
-
Prone positioning in severe ARDS requiring extracorporeal membrane oxygenation.Crit Care. 2020 Jul 8;24(1):397. doi: 10.1186/s13054-020-03110-2. Crit Care. 2020. PMID: 32641155 Free PMC article.
-
Prone positioning during venovenous extracorporeal membrane oxygenation for acute respiratory distress syndrome: a systematic review and meta-analysis.Crit Care. 2021 Aug 12;25(1):292. doi: 10.1186/s13054-021-03723-1. Crit Care. 2021. PMID: 34384475 Free PMC article.
-
Optimizing Management of Acute Respiratory Distress Syndrome in Critically Ill Surgical Patients: A Systematic Review.J Surg Res. 2025 Jan;305:385-397. doi: 10.1016/j.jss.2024.10.039. Epub 2025 Jan 3. J Surg Res. 2025. PMID: 39755005
Cited by
-
Intra-abdominal hypertension and reverse Trendelenburg position increase frontal QRS-T angle in laparoscopic cholecystectomy: An observational study.Medicine (Baltimore). 2025 Mar 14;104(11):e41934. doi: 10.1097/MD.0000000000041934. Medicine (Baltimore). 2025. PMID: 40101078 Free PMC article.
-
Defining the physiological bounds of left ventricular ejection time with a wireless, wearable ultrasound: An analysis of over 137,000 cardiac cycles.Digit Health. 2025 Mar 17;11:20552076251323838. doi: 10.1177/20552076251323838. eCollection 2025 Jan-Dec. Digit Health. 2025. PMID: 40103641 Free PMC article.
References
-
- Combes, A. et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N. Engl. J. Med.378, 1965–1975. 10.1056/NEJMoa1800385 (2018). - PubMed
-
- Bellani, G. et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA315, 788. 10.1001/jama.2016.0291 (2016). - PubMed
-
- Sud, S. et al. Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia: Systematic review and meta-analysis. Intensive Care Med.36, 585–599. 10.1007/s00134-009-1748-1 (2010). - PubMed
-
- Balk, R. A. Positive end-expiratory pressure setting in adults with acute lung injury and acute respiratory distress syndrome: A randomized controlled trial. Yearbook Crit. Care Med.2009, 6–8. 10.1016/S0734-3299(08)79045-2 (2009). - PubMed
-
- Schmid, C. et al. Venovenous extracorporeal membrane oxygenation for acute lung failure in adults. J. Heart Lung Transplantation. 31, 9–15. 10.1016/j.healun.2011.07.013 (2012). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
