

Exploratory testing of functional blood oxygenation level dependent-MRI to image the renoprotective effect of Remote Ischaemic PreConditioning during partial nephrectomy
- PMID: 39738435
- PMCID: PMC11685923
- DOI: 10.1038/s41598-024-83643-6
Exploratory testing of functional blood oxygenation level dependent-MRI to image the renoprotective effect of Remote Ischaemic PreConditioning during partial nephrectomy
Abstract
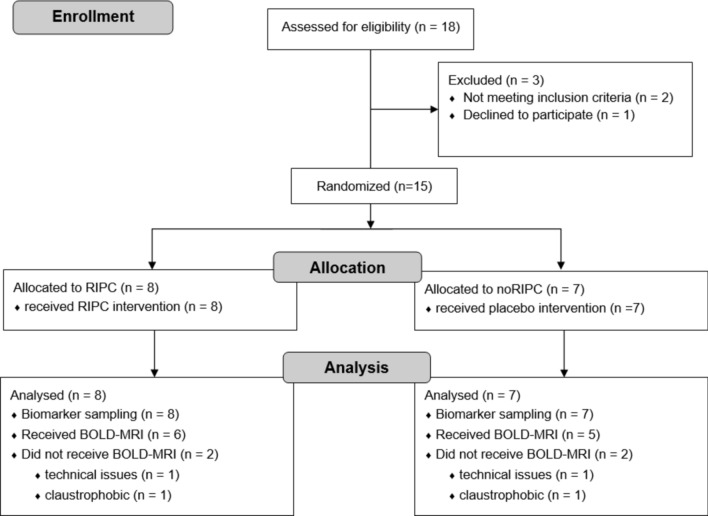
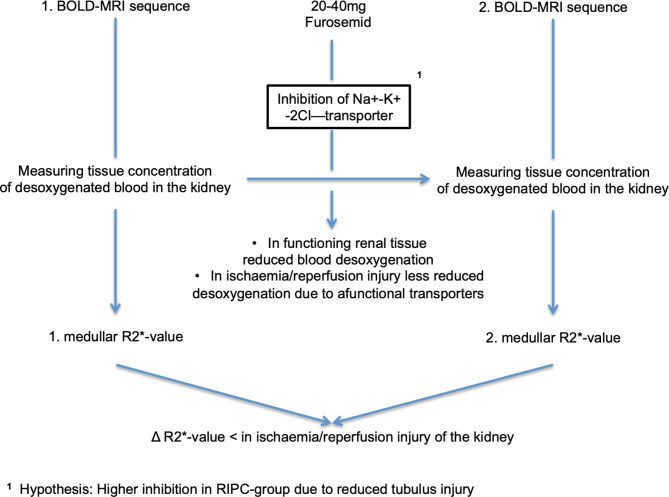
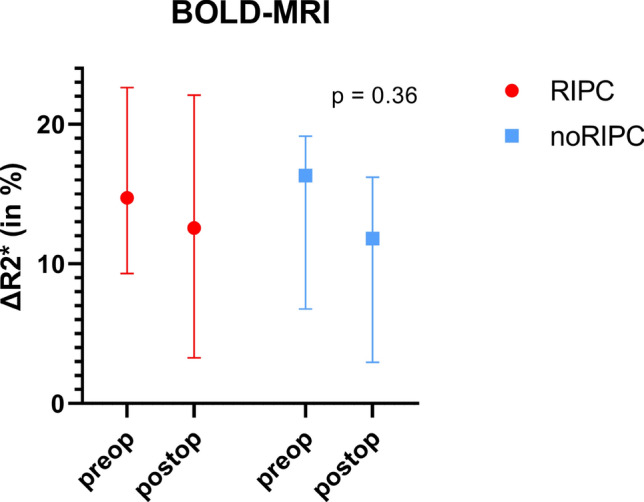
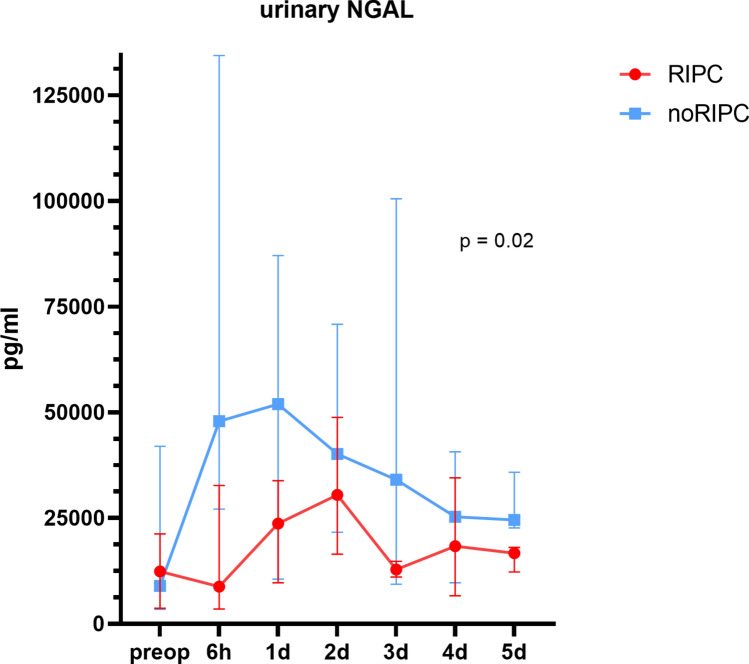
Urinary biomarker studies in cardiothoracic and kidney-sparing surgery have demonstrated renal protection by Remote Ischaemic PreConditioning (RIPC). RIPC intervention generates cycles of ischaemia and reperfusion of the limbs before the actual ischaemia of the target organ (e.g. kidney) is initiated. This explorative trial aims to investigate whether Blood Oxygenation Level Dependent-MRI (BOLD-MRI) can be a suitable technique to image and quantify the renoprotective effect of RIPC on ischaemia/reperfusion injury (IRI) after partial nephrectomy (PN). Overall, 15 patients were enrolled in this randomized controlled trial. Randomization was 1:1, with RIPC in the intervention arm. Urinary neutrophil gelatinase-associated lipocalin (NGAL), a sensitive biomarker for renal tubular damage was measured preoperatively and for the first 5 days after surgery. Functional BOLD-MRI was successfully performed preoperatively and 48 h after PN in 11 patients. BOLD-MRI uses ∆R2* to express acute tubular damage induced by IRI. The more the ∆R2* values have decreased postoperatively, the more damage the renal tubuli have taken. The cumulative urinary concentration of NGAL in the first 5 postoperative days was significantly lower in the RIPC group (p = 0.02) as compared to the control arm, indicating that the RIPC maneuver performed was effective. The highest difference was seen 6 h after surgery with NGAL being 65% lower in the RIPC arm. IRI of the operated kidney expressed by ∆R2* in BOLD-MRI was 2.1 times less pronounced in the RIPC group as compared to the noRIPC group (∆R2* in % preop/postop RIPC: 14.73/12.57 vs. noRIPC 16.33/11.82, p = 0.36). We were able to demonstrate the potential of BOLD-MRI in measuring IRI. For the first time, it was shown that the renoprotective effects of RIPC can be visualized and measured using BOLD-MRI. Larger studies are required to validate these initial findings.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
