

Post mortem cadaveric and imaging mapping analysis of the influence of cochlear implants on cMRI assessment regarding implant positioning and artifact formation
- PMID: 39738529
- PMCID: PMC12122577
- DOI: 10.1007/s00405-024-09164-0
Post mortem cadaveric and imaging mapping analysis of the influence of cochlear implants on cMRI assessment regarding implant positioning and artifact formation
Abstract
Objectives: In times of an aging society and considering the escalating health economic costs, the indications for imaging, particularly magnetic resonance imaging (MRI), must be carefully considered and strictly adhered to. This cadaver study aims to examine the influence of cochlear implant (CI) on the assessment of intracranial structures, artifact formation, and size in cranial MRI (cMRI). Furthermore, it seeks to evaluate the potential limitations in the interpretability and diagnostic value of cMRI in CI patients. Additionally, the study investigates the imaging of the brain stem and the internal ear canal and the feasibility of excluding cholesteatomas in cMRI for CI patients.
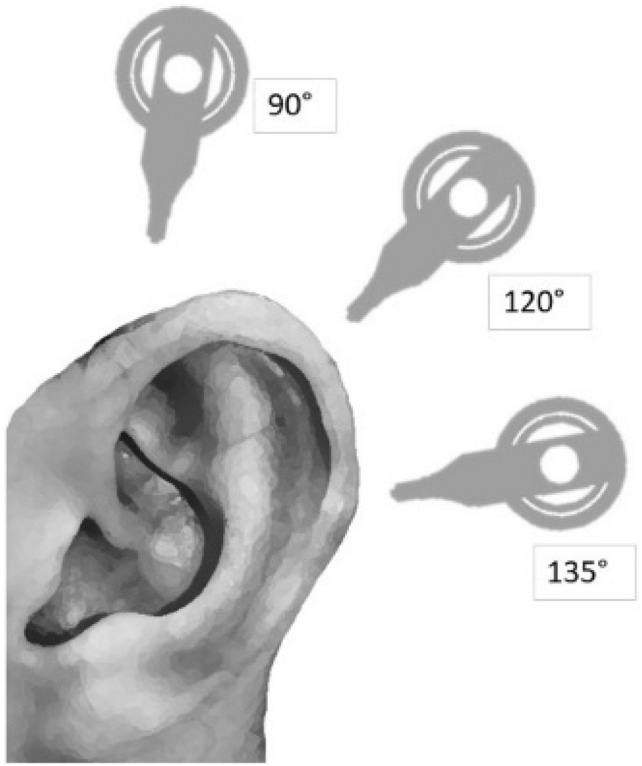
Materials and methods: Two cadaveric specimens were implanted with cochlear implants at varying angular positions (90°, 120°, and 135°), both unilaterally and bilaterally, with and without magnet in situ. MRI acquisition consisted of sequences commonly used in brain MRI scans (T1-MP-RAGE, T2-TSE, T1-TIRM, DWI, CISS). Subsequently, the obtained MRI images were manually juxtaposed with a reference brain from the Computational Anatomy Toolbox CAT12. The size and formation of artifacts were scrutinized to ascertain the assessability of 22 predefined intracranial structures. Furthermore, the internal auditory canal, middle ear and mastoid were evaluated.
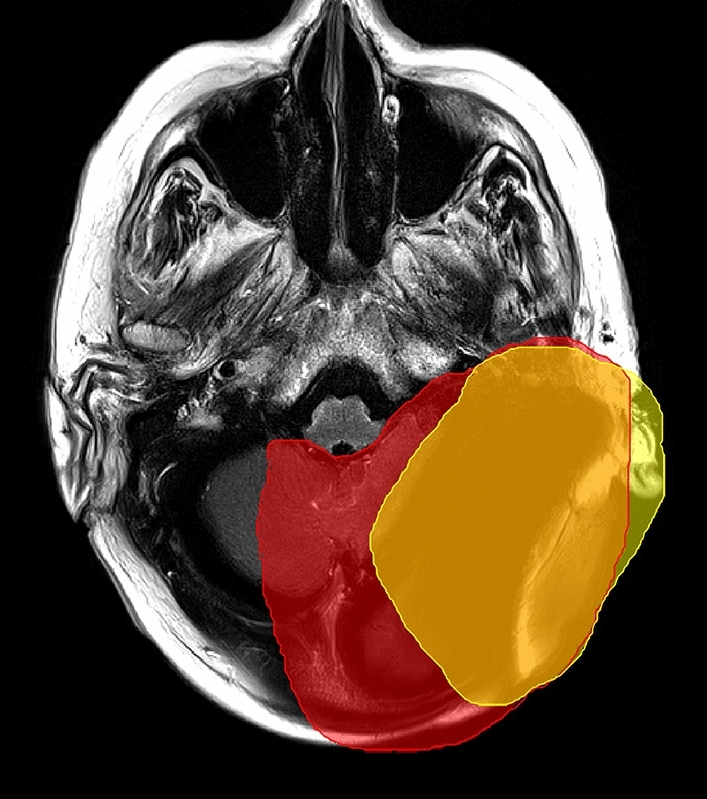
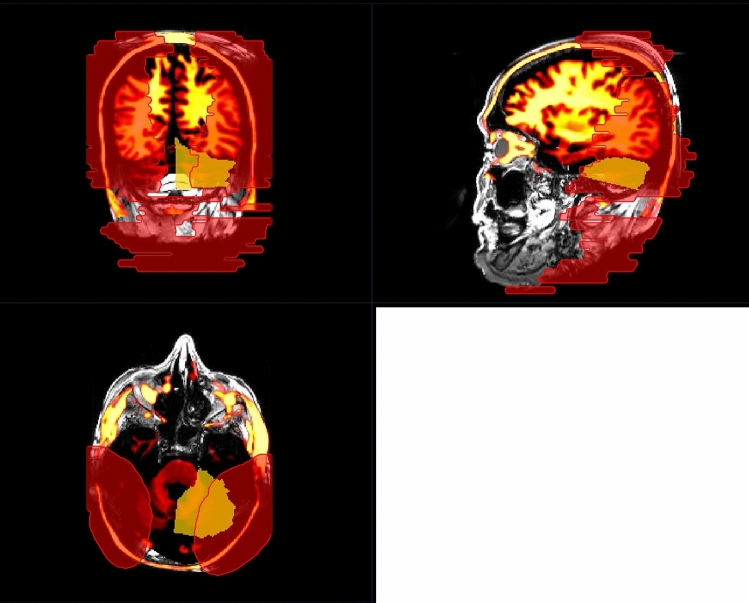
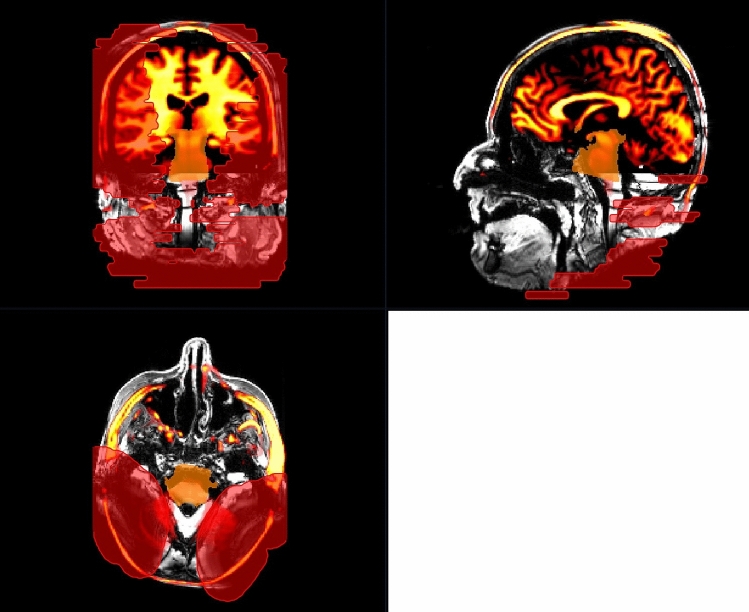
Results: The cadaveric head mapping facilitated the analysis of all 22 predefined intracranial structures. Artifacts were assessed in terms of their minimum and maximum impact on image comparability. Image quality and assessability were stratified into four categories (0-25%, 25-50%, 50-75%, and 75-100% of assessability restriction). The visualization of the central, temporal, parietal, and frontal lobes was contingent upon CI positioning and the choice of imaging sequence. Diffusion-weighted cMRI proved inadequate for monitoring cholesteatoma recurrence in ipsilateral CI patients, regardless of magnet presence. The ipsilateral internal auditory canal was inadequately visualized in both magnet-present and magnet-absent conditions. We divided our results into four categories. Category 3 (orange) indicates considerable limitations, while category 4 (red) indicates no interpretability, as the image is entirely obscured by artifacts.
Conclusion: This study provides detailed predictive power for the assessability and therefore the relevance of performing cMRIs in CI patients. We advocate consulting the relevant CI center if artifact overlay exceeds 50% (categories 3 and 4), to evaluate magnet explantation and reassess the necessity of cMRI. When suspecting cholesteatoma or cholesteatoma recurrences in patients with ipsilateral cochlear implants, diagnostic investigation should preferably be pursued surgically, as the necessary MRI sequences are prone to artifact interference, even in the absence of a magnet. The ipsilateral internal auditory canal remains inadequately evaluable with a magnet in situ, while without the magnet, only rudimentary assessments can be made across most sequences.
Keywords: Artifact; Cochlear implant; Cranial imaging; MRI; Magnet.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: Philipp Arnold and Michael Reich declare no conflict of interest. Antje Aschendorff received travelling expenses and financial support for research from Cochlear Ltd, Australia; financial support for research and travelling expenses from Med-El, Innsbruck, Austria; financial support for research and travelling expenses from Oticon Inc., Somerset, NJ; financial support for research and travelling expenses from Advanced Bionics, Valencia, CA, USA. Susan Arndt received financial support for research and travelling expenses from Cochlear Ltd, Australia; financial support for research and travelling expenses from Med-El, Innsbruck, Austria travelling expenses from Advanced Bionics, Valencia, CA, USA. Manuel Christoph Ketterer received financial support for research from Cochlear Ltd, Australia; financial support for research from Oticon Inc., Somerset, NJ. Research involving human participants: Not applicable.
Figures
Similar articles
-
Magnetic Resonance Imaging Artifact Associated With Transcutaneous Bone Conduction Implants: Cholesteatoma and Vestibular Schwannoma Surveillance.Otolaryngol Head Neck Surg. 2024 Jan;170(1):187-194. doi: 10.1002/ohn.474. Epub 2023 Aug 15. Otolaryngol Head Neck Surg. 2024. PMID: 37582349
-
MRI Artifacts and Cochlear Implant Positioning at 3 T In Vivo.Otol Neurotol. 2015 Jul;36(6):972-6. doi: 10.1097/MAO.0000000000000720. Otol Neurotol. 2015. PMID: 25634466
-
Image Quality and Artifact Reduction of a Cochlear Implant With Rotatable Magnets.Otol Neurotol. 2023 Apr 1;44(4):e223-e229. doi: 10.1097/MAO.0000000000003840. Epub 2023 Feb 20. Otol Neurotol. 2023. PMID: 36806625
-
First MRI With New Cochlear Implant With Rotatable Internal Magnet System and Proposal for Standardization of Reporting Magnet-Related Artifact Size.Otol Neurotol. 2019 Aug;40(7):883-891. doi: 10.1097/MAO.0000000000002269. Otol Neurotol. 2019. PMID: 31219967 Review.
-
MR Imaging and Cochlear Implants with Retained Internal Magnets: Reducing Artifacts near Highly Inhomogeneous Magnetic Fields.Radiographics. 2018 Jan-Feb;38(1):94-106. doi: 10.1148/rg.2018170135. Radiographics. 2018. PMID: 29320320 Review.
Cited by
-
Assessing MRI interpretability of the orbit, paranasal sinuses, and nasopharynx in cochlear implant patients.Front Neurol. 2025 Jul 31;16:1636128. doi: 10.3389/fneur.2025.1636128. eCollection 2025. Front Neurol. 2025. PMID: 40823313 Free PMC article.
References
-
- Arndt S, Aschendorff A, Laszig R, Beck R, Schild C, Kroeger S, Ihorst G, Wesarg T (2011) Comparison of pseudobinaural hearing to real binaural hearing rehabilitation after cochlear implantation in patients with unilateral deafness and tinnitus. Otol Neurotol 32(1):39–47 - PubMed
-
- Canzi P, Aprile F, Simoncelli A, Manfrin M, Magnetto M, Lafe E, Minervini D, Avato I, Terrani S, Scribante A, Gazibegovic D, Benazzo M (2021) MRI-induced artifact by a cochlear implant with a novel magnet system: an experimental cadaver study. Eur Arch Otorhinolaryngol 278(10):3753–3762 - PMC - PubMed
-
- Canzi P, Magnetto M, Simoncelli A, Manfrin M, Aprile F, Lafe E, Carlotto E, Avato I, Scribante A, Preda L, Benazzo M (2022) The role of cochlear implant positioning on MR imaging quality: a preclinical in vivo study with a novel implant magnet system. Eur Arch Otorhinolaryngol 279(6):2889–2898 - PMC - PubMed
-
- Carlson ML, Neff BA, Link MJ, Lane JI, Watson RE, McGee KP, Bernstein MA, Driscoll CL (2015) Magnetic resonance imaging with cochlear implant magnet in place: safety and imaging quality. Otol Neurotol 36:965–971 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
