

Vitamin D: an important treatment for secondary hyperparathyroidism in chronic kidney disease?
- PMID: 39738859
- PMCID: PMC12049386
- DOI: 10.1007/s11255-024-04334-9
Vitamin D: an important treatment for secondary hyperparathyroidism in chronic kidney disease?
Abstract
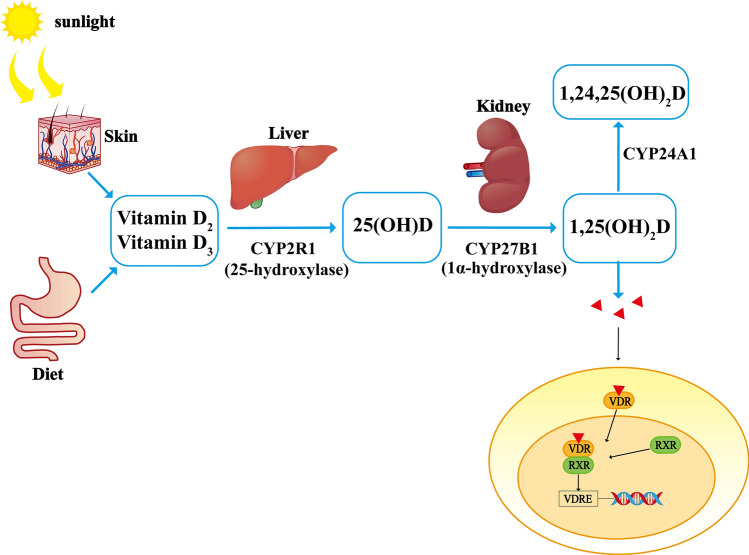
Secondary hyperparathyroidism (SHPT) is one of the most common complications of chronic kidney disease (CKD). Vitamin D levels begin to decrease in the early stages of CKD, and these vitamin D-related changes play a central role in the occurrence and development of SHPT. Vitamin D-based drugs, which inhibit parathyroid hormone secretion either directly or indirectly, are commonly used to treat SHPT. However, vitamin D-based drugs can also lead to a dysregulated balance between serum calcium and phosphorus, as well as other adverse reactions. Over the past several decades, researchers have conducted in-depth studies on the pathogenesis of SHPT, developed new vitamin D-based drugs, and explored combinatory methods to improve treatment efficacy for the disease. Here, we review vitamin D metabolism, the diagnosis of vitamin D deficiency in patients with CKD, the pathogenesis of SHPT, the pharmacological effects of vitamin D drugs, and the benefits and side effects of using vitamin D to treat SHPT.
Keywords: Chronic kidney disease; Complication; Mechanism; Secondary hyperparathyroidism; Treatment; Vitamin D.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interest: The authors declare no competing interests.
Figures

Similar articles
-
Outcomes of secondary hyperparathyroidism in chronic kidney disease and the direct costs of treatment.J Manag Care Pharm. 2007 Jun;13(5):397-411. doi: 10.18553/jmcp.2007.13.5.397. J Manag Care Pharm. 2007. PMID: 17605511 Free PMC article. Review.
-
Current treatment options for secondary hyperparathyroidism in patients with stage 3 to 4 chronic kidney disease and vitamin D deficiency.Expert Opin Drug Saf. 2021 Nov;20(11):1333-1349. doi: 10.1080/14740338.2021.1931117. Epub 2021 Jun 9. Expert Opin Drug Saf. 2021. PMID: 33993809 Review.
-
Rationale for Raising Current Clinical Practice Guideline Target for Serum 25-Hydroxyvitamin D in Chronic Kidney Disease.Am J Nephrol. 2019;49(4):284-293. doi: 10.1159/000499187. Epub 2019 Mar 15. Am J Nephrol. 2019. PMID: 30878999 Clinical Trial.
-
Management of secondary hyperparathyroidism in stages 3 and 4 chronic kidney disease.Endocr Pract. 2008 Jan-Feb;14(1):18-27. doi: 10.4158/EP.14.1.18. Endocr Pract. 2008. PMID: 18238737 Review.
-
Extended-release calcifediol in stage 3-4 chronic kidney disease: a new therapy for the treatment of secondary hyperparathyroidism associated with hypovitaminosis D.J Nephrol. 2022 Apr;35(3):863-873. doi: 10.1007/s40620-021-01152-5. Epub 2021 Oct 9. J Nephrol. 2022. PMID: 34626363 Free PMC article. Review.
Cited by
-
Beyond blood pressure: identifying factors associated with rapid kidney function decline in patients with CKD and coexisting COPD.Int Urol Nephrol. 2025 Jun;57(6):1985-1986. doi: 10.1007/s11255-024-04325-w. Epub 2024 Dec 19. Int Urol Nephrol. 2025. PMID: 39699841 No abstract available.
-
Harnessing AI for real-time monitoring and precision medicine: enhancing cardiovascular risk prediction in CKD management through panimmune-inflammation value.Int Urol Nephrol. 2025 Aug;57(8):2723-2724. doi: 10.1007/s11255-025-04482-6. Epub 2025 Apr 1. Int Urol Nephrol. 2025. PMID: 40164857 No abstract available.
-
Improving search strategies in bibliometric studies on machine learning in renal medicine.Int Urol Nephrol. 2025 Jun;57(6):1987-1988. doi: 10.1007/s11255-024-04335-8. Epub 2024 Dec 23. Int Urol Nephrol. 2025. PMID: 39714749
References
-
- Liyanage T, Ninomiya T, Jha V, Neal B, Patrice HM, Okpechi I et al (2015) Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet Lond Engl 385:1975–1982 - PubMed
-
- Goodman WG, Quarles LD (2008) Development and progression of secondary hyperparathyroidism in chronic kidney disease: lessons from molecular genetics. Kidney Int 74:276–288. https://linkinghub.elsevier.com/retrieve/pii/S0085253815532997 - PubMed
-
- Ronco C, Cozzolino M (2012) Mineral metabolism abnormalities and vitamin D receptor activation in cardiorenal syndromes. Heart Fail Rev 17:211–220. 10.1007/s10741-011-9232-8 - PubMed
-
- Stevens PE (2013) Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice Guideline. Ann Intern Med 158:825. 10.7326/0003-4819-158-11-201306040-00007 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
