

Understanding MASH: An Examination of Progression and Clinical Outcomes by Disease Severity in the TARGET-NASH Database
- PMID: 39739194
- PMCID: PMC11787050
- DOI: 10.1007/s12325-024-03085-4
Understanding MASH: An Examination of Progression and Clinical Outcomes by Disease Severity in the TARGET-NASH Database
Abstract
Introduction: Metabolic dysfunction-associated steatohepatitis (MASH), the progressive form of metabolic dysfunction-associated steatotic liver disease (MASLD), is linked to cardiometabolic risk factors such as obesity and type 2 diabetes (T2D). The rising prevalence of MASH and risk of hepatic and extra-hepatic complications emphasize the need for a better understanding of disease progression and associated outcomes. This study aimed to evaluate the incidence of, and demographic and clinical characteristics associated with, progression to MASH-related complications by disease severity in patients with non-cirrhotic MASH or MASH cirrhosis. Alignment between noninvasive tests (NITs) and biopsy-determined fibrosis stage was also assessed.
Methods: This analysis used data from the TARGET-NASH cohort that includes adults with MASH across academic and community sites in the United States. Patients with non-cirrhotic MASH or MASH cirrhosis were stratified by disease severity based on fibrosis stage or cirrhosis. Progression to MASH-related outcomes, including all-cause mortality, cirrhosis, and liver transplantation, was assessed.
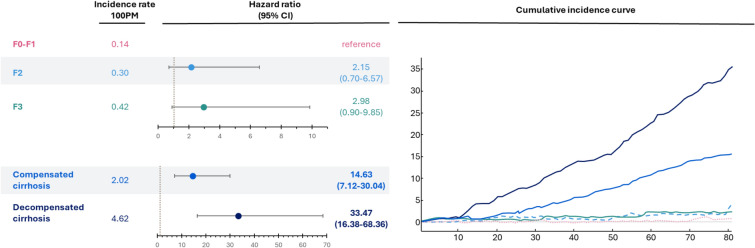
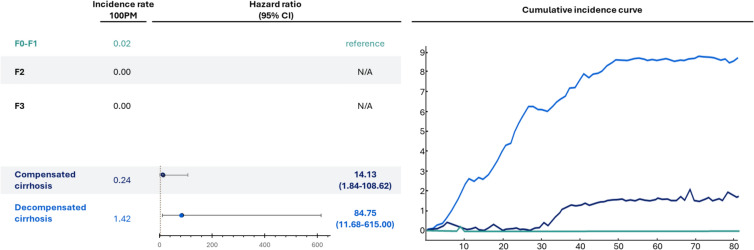
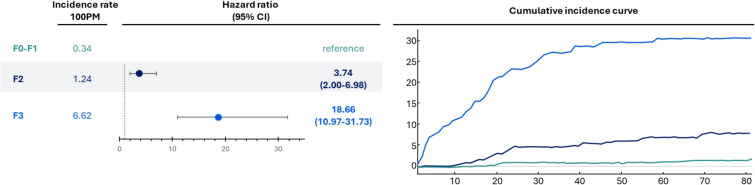
Results: Among the 2378 patients included in this analysis, 48% had MASH cirrhosis. Incidence of all-cause mortality increased with disease severity from 0.14/100 person-months (100PM) at fibrosis stage 0-1 (F0-F1) to 2.02/100PM with compensated cirrhosis and 4.62/100PM with decompensated cirrhosis. Compared with patients with F0-F1, risk of progression to cirrhosis was higher in patients with F3 [hazard ratio (HR), 95% confidence interval (CI); 18.66, 10.97-31.73] and F2 (HR, 95% CI; 3.74, 2.00-6.98). Among those who progressed to MASH-related outcomes, 67.9% had T2D and 73.9% had hypertension. Vibration-controlled transient elastography showed better alignment with biopsy-determined fibrosis stage than Fibrosis-4 Index (FIB-4).
Conclusions: Progression to all-cause mortality in patients with MASH was significantly associated with the presence of higher fibrosis stage and cirrhosis. Cardiometabolic comorbidities such as T2D and hypertension were prevalent in patients with MASH progression. Early identification and management of MASH may mitigate disease progression and liver-related complications.
Keywords: Cirrhosis; Disease progression; Fibrosis; Metabolic dysfunction-associated steatohepatitis (MASH); Noninvasive test (NIT).
Plain language summary
Metabolic dysfunction-associated steatotic liver disease is a common liver condition linked to metabolic health problems such as obesity and type 2 diabetes. Metabolic dysfunction-associated steatohepatitis (MASH) is a severe form of this condition characterized by liver inflammation and damage that can progress to cirrhosis, or scarring of the liver. Data from the TARGET-NASH cohort were analyzed to understand how MASH progresses and affects people’s health over time as well as the demographic and clinical characteristics of those who experience MASH progression. Patients were divided into groups based on severity of liver damage determined by fibrosis stage or cirrhosis. The study found that people with more severe liver damage (higher stage of fibrosis or cirrhosis) had a higher risk of serious health outcomes such as worsening liver damage, the need for a liver transplant, or death.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: Aarth Sheth, PharmD and Rakesh Luthra, MS are employees of Novo Nordisk Inc. Ethical Approval: This article is based on analyses of previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors. Additional Information: The manuscript uses data collected in TARGET-NASH (NCT02815891).
Figures
Similar articles
-
EASL-EASD-EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD): Executive Summary.Diabetologia. 2024 Nov;67(11):2375-2392. doi: 10.1007/s00125-024-06196-3. Diabetologia. 2024. PMID: 38869512 Free PMC article.
-
EASL-EASD-EASO Clinical Practice Guidelines on the Management of Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD).Obes Facts. 2024;17(4):374-444. doi: 10.1159/000539371. Epub 2024 Jun 7. Obes Facts. 2024. PMID: 38852583 Free PMC article.
-
Noninvasive identification of metabolic dysfunction-associated steatohepatitis (INFORM MASH): a retrospective cohort and disease modeling study.Expert Rev Gastroenterol Hepatol. 2025 Apr;19(4):427-435. doi: 10.1080/17474124.2025.2477249. Epub 2025 Mar 21. Expert Rev Gastroenterol Hepatol. 2025. PMID: 40067340
-
NAFLD (MASLD)/NASH (MASH): Does It Bother to Label at All? A Comprehensive Narrative Review.Int J Mol Sci. 2024 Aug 2;25(15):8462. doi: 10.3390/ijms25158462. Int J Mol Sci. 2024. PMID: 39126031 Free PMC article. Review.
-
Noninvasive Tests to Assess Fibrosis and Disease Severity in Metabolic Dysfunction-Associated Steatotic Liver Disease.Semin Liver Dis. 2024 Aug;44(3):287-299. doi: 10.1055/s-0044-1788277. Epub 2024 Jul 9. Semin Liver Dis. 2024. PMID: 38981691 Review.
References
-
- Barritt AS, Yu F, Mospan AR, et al. High concordance between nonalcoholic fatty liver disease and metabolic dysfunction-associated steatotic liver disease in the TARGET-NASH real-world cohort. Am J Gastroenterol. 2024;119(8):1624–7. - PubMed
-
- Le P, Chaitoff A, Rothberg MB, et al. Population-based trends in prevalence of nonalcoholic fatty liver disease in US adults with type 2 diabetes. Clin Gastroenterol Hepatol. 2019;17(11):2377–8. - PubMed
-
- Harrison SA, Gawrieh S, Roberts K, et al. Prospective evaluation of the prevalence of non-alcoholic fatty liver disease and steatohepatitis in a large middle-aged US cohort. J Hepatol. 2021;75(2):284–91. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
