

Treatment strategies to reduce cardiovascular risk in persons with chronic kidney disease and Type 2 diabetes
- PMID: 39739537
- PMCID: PMC12033002
- DOI: 10.1111/joim.20050
Treatment strategies to reduce cardiovascular risk in persons with chronic kidney disease and Type 2 diabetes
Abstract
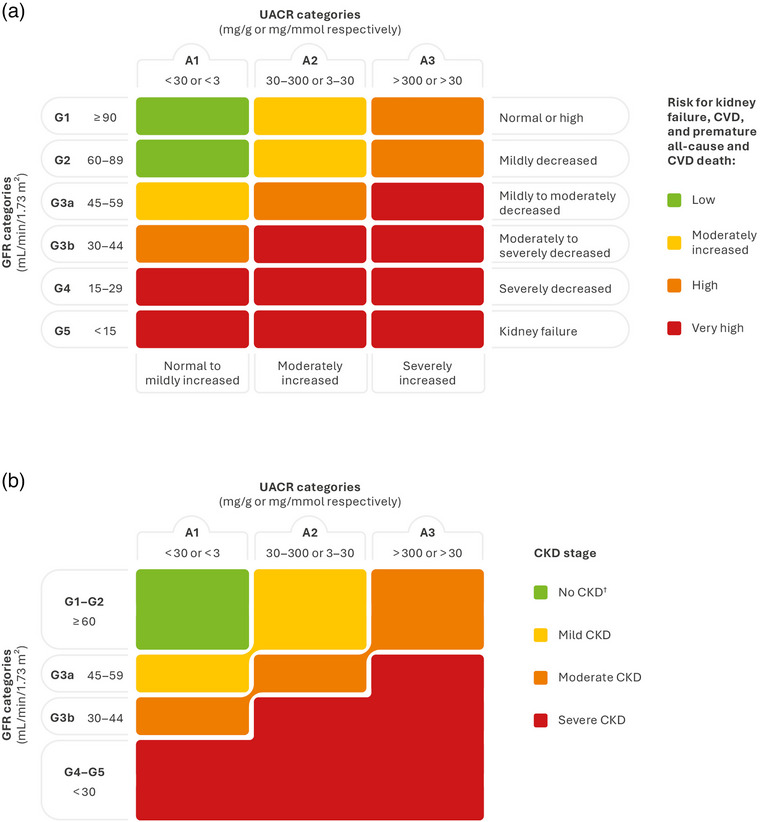
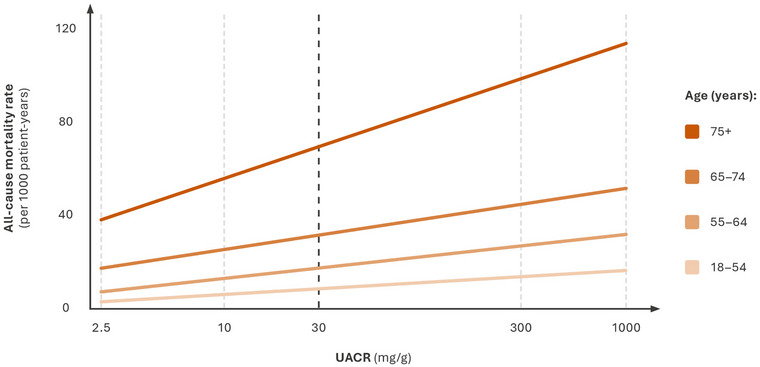
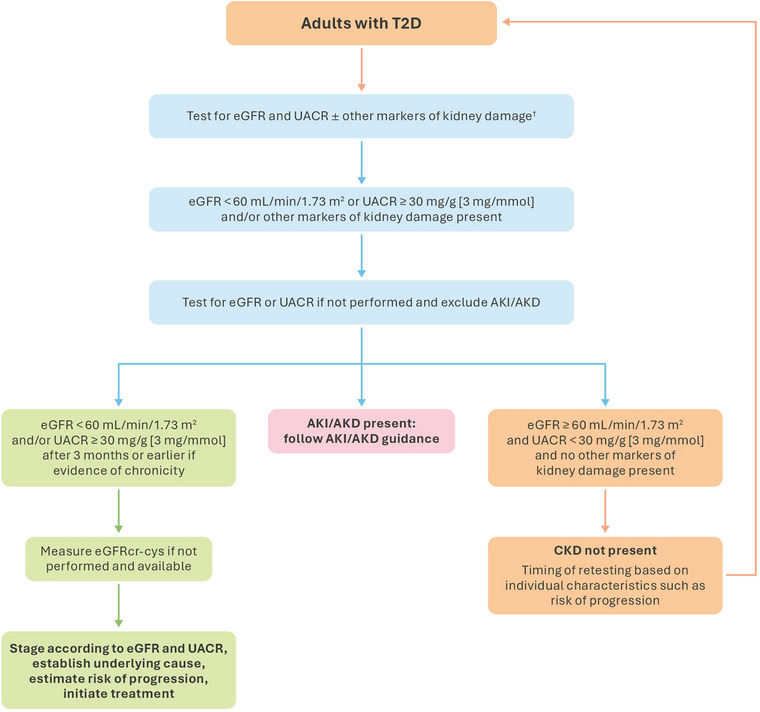
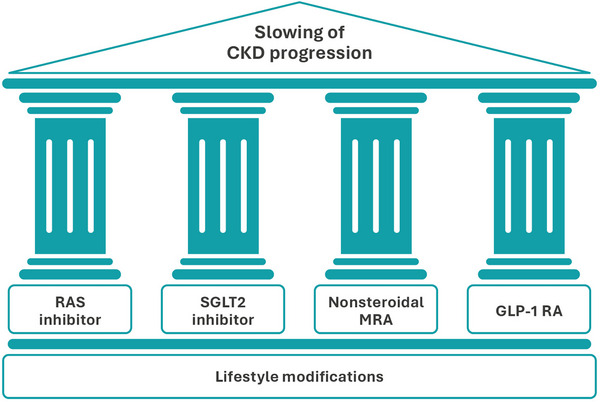
Chronic kidney disease (CKD) is a prevalent and progressive condition associated with significant mortality and morbidity. Diabetes is a common cause of CKD, and both diabetes and CKD increase the risk of cardiovascular disease (CVD), the leading cause of death in individuals with CKD. This review will discuss the importance of early detection of CKD and prompt pharmacological intervention to slow CKD progression and delay the development of CVD for improving outcomes. Early CKD is often asymptomatic, and diagnosis usually requires laboratory testing. The combination of estimated glomerular filtration rate (eGFR) and urine albumin-to-creatinine ratio (UACR) measurements is used to diagnose and determine CKD severity. Guidelines recommend at least annual screening for CKD in at-risk individuals. While eGFR testing rates are consistently high, rates of UACR testing remain low. This results in underdiagnosis and undertreatment of CKD, leaving many individuals at risk of CKD progression and CVD. UACR testing is an actionable component of the CKD definition. A four-pillar treatment approach for slowing the progression of diabetic kidney disease is suggested, comprising a renin-angiotensin-system (RAS) inhibitor, a sodium-glucose cotransporter 2 inhibitor, a glucagon-like peptide 1 receptor agonist, and the nonsteroidal mineralocorticoid receptor antagonist finerenone. The combination of these agents provides a greater cardiorenal risk reduction compared with RAS inhibitors alone. Early detection of CKD and prompt intervention with guideline-directed medical therapy are crucial for reducing CVD risk in individuals with CKD and diabetes. Evidence from ongoing studies will advance our understanding of optimal therapy in this population.
Keywords: Type 2 diabetes; cardiovascular risk factors; kidney disease.
© 2025 The Author(s). Journal of Internal Medicine published by John Wiley & Sons Ltd on behalf of Association for Publication of The Journal of Internal Medicine.
Conflict of interest statement
Dr Zannad reports personal fees from 89Bio, Abbott, Acceleron, Applied Therapeutics, Bayer, Betagenon, Boehringer Ingelheim, BMS, CVRx, Cambrian, Cardior, Cereno pharmaceutical, Cell Prothera, CEVA, Inventiva, KBP, Merck, Novo Nordisk, Owkin, Otsuka, Roche Diagnostics, Northsea, USa2, having stock options at G3Pharmaceutical and equities at Cereno, Cardiorenal, Eshmoun Clinical Research, and being the founder of Cardiovascular Clinical Trialists.
Dr McGuire reports consulting fees from Boehringer Ingelheim, Lilly USA, Novo Nordisk, AstraZeneca, Lexicon Pharmaceuticals, Pfizer, Applied Therapeutics, Altimmune, Bayer, Neurotronics, Intercept Pharmaceuticals, Esperion, Ventyx Pharmaceuticals, New Amsterdam, CSL Behring, and Amgen.
Professor Ortiz has received grants from Sanofi and consultancy or speaker fees or travel support from Adviccene, Alexion, Astellas, AstraZeneca, Amicus, Amgen, Bioporto, Boehringer Ingelheim, Fresenius Medical Care, GSK, Bayer, Sanofi‐Genzyme, Sobi, Menarini, Mundipharma, Kyowa Kirin, Lilly, Freeline, Idorsia, Chiesi, Otsuka, Novo Nordisk, Sysmex and Vifor Fresenius Medical Care Renal Pharma and Spafarma and is Director of the Catedra UAM‐Mundipharma research collaboration for diabetic kidney disease and the Catedra UAM–AstraZeneca research collaboration for chronic kidney disease and electrolytes. He is a member of the European Renal Association Council and SOMANE. He has stock in Telara Farma.
Figures
Similar articles
-
Combination therapy: an upcoming paradigm to improve kidney and cardiovascular outcomes in chronic kidney disease.Nephrol Dial Transplant. 2025 Feb 5;40(Supplement_1):i3-i17. doi: 10.1093/ndt/gfae212. Nephrol Dial Transplant. 2025. PMID: 39907543 Free PMC article. Review.
-
Non-steroidal mineralocorticoid antagonists and hyperkalemia monitoring in chronic kidney disease patients associated with type II diabetes: a narrative review.Postgrad Med. 2024 Mar;136(2):111-119. doi: 10.1080/00325481.2024.2316572. Epub 2024 Feb 16. Postgrad Med. 2024. PMID: 38344772 Review.
-
Finerenone and Heart Failure Outcomes by Kidney Function/Albuminuria in Chronic Kidney Disease and Diabetes.JACC Heart Fail. 2022 Nov;10(11):860-870. doi: 10.1016/j.jchf.2022.07.013. Epub 2022 Oct 12. JACC Heart Fail. 2022. PMID: 36328655 Clinical Trial.
-
Management of chronic kidney disease in type 2 diabetes: screening, diagnosis and treatment goals, and recommendations.Postgrad Med. 2022 May;134(4):376-387. doi: 10.1080/00325481.2021.2009726. Epub 2021 Dec 29. Postgrad Med. 2022. PMID: 34817311 Review.
-
The dapagliflozin and prevention of adverse outcomes in chronic kidney disease (DAPA-CKD) trial: baseline characteristics.Nephrol Dial Transplant. 2020 Oct 1;35(10):1700-1711. doi: 10.1093/ndt/gfaa234. Nephrol Dial Transplant. 2020. PMID: 32862232 Free PMC article. Clinical Trial.
Cited by
-
Prognosis of non-albuminuric patients with the cardiovascular-kidney-metabolic syndrome.Clin Kidney J. 2025 Mar 12;18(4):sfaf074. doi: 10.1093/ckj/sfaf074. eCollection 2025 Apr. Clin Kidney J. 2025. PMID: 40226369 Free PMC article.
References
-
- Jager KJ, Kovesdy C, Langham R, Rosenberg M, Jha V, Zoccali C. A single number for advocacy and communication‐worldwide more than 850 million individuals have kidney diseases. Kidney Int. 2019;96(5):1048–1050. - PubMed
-
- Foreman KJ, Marquez N, Dolgert A, Fukutaki K, Fullman N, McGaughey M, et al. Forecasting life expectancy, years of life lost, and all‐cause and cause‐specific mortality for 250 causes of death: reference and alternative scenarios for 2016–40 for 195 countries and territories. Lancet. 2018;392(10159):2052–2090. - PMC - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group . KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2024;105(4S):S117–S314. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
