

Adjuvant Intensity Modulated Radiation Therapy With a Pedicled Flap Reconstruction in Oral Cavity Squamous Cell Carcinomas: Implications on Target Delineation
- PMID: 39739551
- PMCID: PMC12248275
- DOI: 10.1002/hed.28056
Adjuvant Intensity Modulated Radiation Therapy With a Pedicled Flap Reconstruction in Oral Cavity Squamous Cell Carcinomas: Implications on Target Delineation
Abstract
Objectives: To address controversies regarding target volume delineation for adjuvant intensity-modulated radiation therapy for oral cavity squamous cell carcinoma with pedicled flap reconstruction and elective nodal irradiation (ENI).
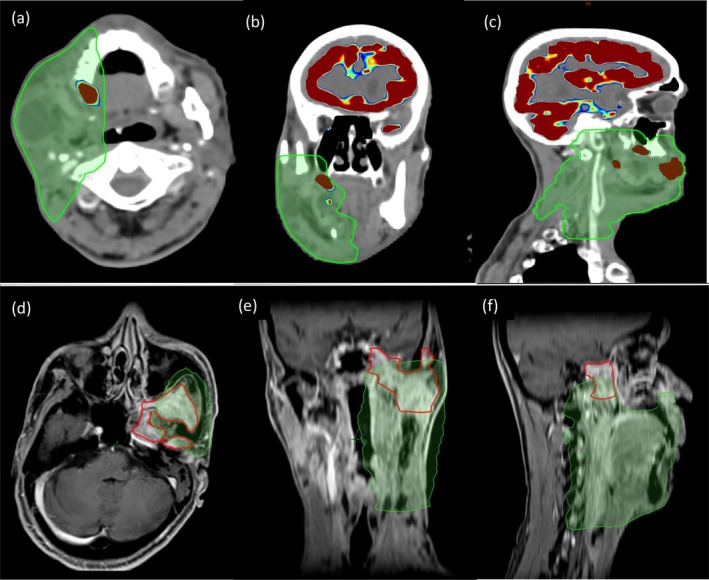
Materials and methods: During target volume delineation, the primary tumor bed was the pre-surgical gross tumor volume with an additional isotropic margin of 5-10 mm. Additionally, the flap and body tissue junction were given a margin of 5-10 mm (if not already given). An effort was not made to trace the flap for inclusion in the clinical target volume (CTV), except when it traversed through the involved nodal regions. Contralateral ENI was carried out only in tumors crossing the midline when there was a heavy nodal burden at Ia/Ib.
Results: In the 143 patients analyzed, the most common sub-site was buccal mucosa (78, 54.5%). Contralateral ENI was done in 63 patients (36 Tongue, 23 Buccoalveolar). The median follow-up of surviving patients was 24 months. The 2-year Locoregional Control, Disease-Free Survival, and Overall Survival were 77.4%, 64.5%, and 79% respectively. Overall, there were 55 (38.5%) recurrences, of which 35 (24.5%) were either local, regional, or combined locoregional failures, 13 (9.1%) were distant failures alone, and 7 (4.9%) had both locoregional and distant failures. The elective nodal regions had 3 (2.1%) contralateral nodal failures.
Conclusion: The entire flap need not be intentionally covered in the target volume. Contralateral ENI should be considered only for patients with heavy nodal burden at ipsilateral level Ia/Ib, in tumors crossing the midline, or in tumors having a high propensity for contralateral lymph nodal involvement.
© 2024 The Author(s). Head & Neck published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


Similar articles
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Minimally invasive surgery versus radiotherapy/chemoradiotherapy for small-volume primary oropharyngeal carcinoma.Cochrane Database Syst Rev. 2016 Dec 11;12(12):CD010963. doi: 10.1002/14651858.CD010963.pub2. Cochrane Database Syst Rev. 2016. PMID: 27943254 Free PMC article.
-
Analysis of clinicopathological factors associated with recurrence after post operative radiotherapy in oral cavity squamous cell carcinoma.J Cancer Res Ther. 2025 Apr 1;21(3):558-566. doi: 10.4103/jcrt.jcrt_1425_24. Epub 2025 Jul 5. J Cancer Res Ther. 2025. PMID: 40616537
-
Interventions for the treatment of oral cavity and oropharyngeal cancer: chemotherapy.Cochrane Database Syst Rev. 2011 Apr 13;(4):CD006386. doi: 10.1002/14651858.CD006386.pub3. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2021 Dec 20;12:CD006386. doi: 10.1002/14651858.CD006386.pub4. PMID: 21491393 Updated.
-
Interventions for the treatment of oral and oropharyngeal cancers: targeted therapy and immunotherapy.Cochrane Database Syst Rev. 2015 Dec 1;2015(12):CD010341. doi: 10.1002/14651858.CD010341.pub2. Cochrane Database Syst Rev. 2015. PMID: 26625332 Free PMC article.
References
-
- Pignon J. P., Maitre A. l., Maillard E., Bourhis J., and MACH‐NC Collaborative Group , “Meta‐Analysis of Chemotherapy in Head and Neck Cancer (MACH‐NC): An Update on 93 Randomised Trials and 17,346 Patients,” Radiotherapy and Oncology 92, no. 1 (2009): 4–14, 10.1016/j.radonc.2009.04.014. - DOI - PubMed
-
- Gupta T., Kannan S., Ghosh‐Laskar S., and Agarwal J. P., “Systematic Review and Meta‐Analyses of Intensity‐Modulated Radiation Therapy Versus Conventional Two‐Dimensional and/or or Three‐Dimensional Radiotherapy in Curative‐Intent Management of Head and Neck Squamous Cell Carcinoma,” PLoS One 13, no. 7 (2018): e0200137, 10.1371/journal.pone.0200137. - DOI - PMC - PubMed
-
- Gregoire V., Evans M., Le Q. T., et al., “Delineation of the Primary Tumour Clinical Target Volumes (CTV‐P) in Laryngeal, Hypopharyngeal, Oropharyngeal and Oral Cavity Squamous Cell Carcinoma: AIRO, CACA, DAHANCA, EORTC, GEORCC, GORTEC, HKNPCSG, HNCIG, IAG‐KHT, LPRHHT, NCIC CTG, NCRI, NRG Oncology, PHNS, SBRT, SOMERA, SRO, SSHNO, TROG Consensus Guidelines,” Radiotherapy and Oncology 126, no. 1 (2018): 3–24, 10.1016/j.radonc.2017.10.016. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
